

Unsafe abortion is one of the major causes of maternal mortality that accounts for approximately 4.7%–13.2% maternal deaths every year (Say et al, 2014). In developing countries, every year, nearly seven million women get admitted in hospitals for the treatment of complications related to unsafe abortion (Singh, 2016). Some of the complications that can occur as a result of unsafe abortion include haemorrhage, infection, uterine perforation, and injury to the genital tract and internal organs that can be life threatening to women (World Health Organization [WHO], 2019).
Overview of abortion
Induced abortions are a major cause of concern worldwide. According to the WHO, on average, 56 million induced abortions took place around the globe between 2010–2014; which formed 25% of all pregnancies (WHO, 2019). Induced abortions carry minimal risk, if performed as per the WHO recommended guidelines and methods for safe abortion. On the contrary, if they are performed by an untrained provider, who lacks the necessary skills, or are done in an environment that does not follow the minimal medical quality standards, they are considered as unsafe abortion (WHO, 2012). Ganatra and colleagues (2017) reported that 25 million unsafe abortions took place worldwide between 2010–2014; out of which almost 88% occurred in the developing countries. More than half of all the estimated unsafe abortions, globally, were performed in Asia, mostly in south and central Asia (Ganatra et al, 2017).
The case of Pakistan
Pakistan is amongst the countries with a high fertility rate of 3.6 births per woman (National Institute of Population Studies [NIPS], 2019). Pakistan Demographic and Health Survey (PDHS) reveals a gradual, but very slow, decline in the fertility rate in the last three decades, from 5.4 births per woman, in 1990–1991, to 3.8 in 2012–2013, and 3.6 births per woman, in 2017–2018 (NIPS, 2019). Among these pregnancies, many fall in the category of unintended pregnancies. One of the major reasons behind the of high burden of unintended pregnancies in Pakistan is the low contraceptive prevalence rate (34%), with 25% of the couples using modern methods and 9% using traditional methods (NIPS, 2019). The high unmet need for family planning, that is, 20%, is with regard to reproductive age women who are not using contraception but wish to postpone or limit pregnancy (NIPS, 2019).
PPakistan is also suffering from a high burden of unintended pregnancies and induced abortions. Almost half of pregnancies, that is 46% of the total nine million pregnancies that occurred in 2012 in Pakistan, were unintended; out of which more than half, 25% (estimated 2.25 million), were intentionally terminated (Sathar et al, 2014). The majority of these abortions were among the poor rural women and were performed by untrained providers, such as traditional birth attendants (TBAs), under unsafe and unhygienic conditions (Guttmacher Institute and Population Council, 2013), and later many of these were presented at health facilities for the treatment of complications (Sathar et al, 2013).
In Pakistan, the abortion law has undergone several amendments since 1990. Until 1990, the Pakistan Penal Code criminalised abortion, unless it was performed in ‘good faith to save the woman's life’. This amendment was meant to ensure conformity with the injunctions of Islam, in line with the guidance in the Holy Quran and Sunnah. In 1997, as a result of the amendment of the Penal Code, widened legal permission was granted to carry out abortion in the early stages of pregnancy, not only to ‘save the life of the woman’ but also to provide ‘necessary treatment’ (Ipas, 2020). However, inaccurate and incomplete knowledge and interpretation by the healthcare providers, and the community at large, significantly affects timely and appropriate decision-making (Shah et al, 2014). This further complicates accessibility to available safe abortion care services provided by competent Healthcare professionals (Zaidi, 2014).
Determinants of induced abortions
There are several determinants of induced abortions. One of the major factors is unintended pregnancy due to low prevalence of contraceptive use in the country, leading to high unmet need for family planning (Sathar et al, 2014; Naveed et al, 2016; Sultana et al, 2019). A hospital-based, cross-sectional survey of 3 010 pregnant women in Sindh found that 38% of the women had unintended pregnancies as a result of no or minimum utilisation of contraceptive methods (Habib et al, 2017). Other main reasons found related to low usage of contraceptive methods were: dissatisfaction of spouse with condoms, unawareness about the methods, ignorance about and dissatisfaction with the method due to side effects (Naveed et al, 2016) and contraceptive failure (Khurshid and Syed, 2019).
Another determinant is the desire for a small family size based on the sex of the child. With time, small nuclear families are preferred over large extended families due to increasing inflationary tendencies. With an increased desire for a small family size, there is also a need to control the sex of the children. Sex ratio at birth (SRB) in Pakistan is 1.087 above the expected biological ratio of less than 1.08 (World Bank, 2019). The UN estimates for SRB predict the ratio to be the same in the next five years as well (World Bank, 2019). Sex selective abortions are, therefore, a key factor that can lead to induced abortions. The sex of a baby can be easily identified with the help of technology (Qayyum and Rehan, 2017); considering the difference in the sex ratio at birth, it is possible that services for induced abortion are requested in case the baby is not of the preferred sex (Channon, 2017). A cross-sectional survey conducted in six cities in three provinces of Pakistan reported that almost 35% of the 968 women opted for induced abortion after conceiving a female child (Qayyum and Rehan, 2017).
Another reason identified by Avais and colleagues (2016) was having too many children in the family. Women in their study shared that they already had the desired number of children and, therefore, opted for induced abortion. One more reason, reported in another study, for opting induced abortion was that women who already had the desired number of children, were not psychologically prepared to have another pregnancy (Khurshid and Syed, 2019).
In low-income families, the economic situation also pressurises couples to choose abortion (Naveed et al, 2016). A study conducted in Multan on women admitted in the emergency department of a tertiary care hospital with complications of induced abortion reported that approximately 70% of the 296 women were from a low socioeconomic background and were concerned about increased financial burden with the addition of more family members (Zafar et al, 2018).
Literature also highlights that induced abortions for unwanted pregnancies are usually opted by those females who are pregnant from pre- or extra-marital relationships (Avais et al, 2016; Naveed et al, 2016), or those who are commercial sex workers (Avais et al, 2016), or have a history of intimate partner violence (Zakar et al, 2016). Hence, under the influence of the aforementioned determinants, there is a considerable increase in induced abortions, leading to higher number of morbidities and mortalities related to unsafe abortion procedures.
Barriers to safe abortions in Pakistan
The majority of the women in Pakistan cannot access safe abortion services due to certain barriers that prevail in the country. Firstly, despite several amendments in the country's abortion law, there are still different interpretations regarding this law in the country, which sometimes restrict access to safe abortion services for women (Guttmacher Institute and Population Council, 2013). Due to inappropriate interpretations of the country's law, many women opt for unsafe abortions and approach traditional birth attendants (Dai) who provide clandestine procedures endangering women's lives (Naveed et al, 2016).
On the other hand, trained healthcare providers often demonstrate a negative attitude towards women seeking abortion due to their conflicting personal and professional values (Kristen et al, 2011) and also their limited knowledge and skills regarding the safe abortion methods recommended by WHO (Baig et al, 2017). Most healthcare professionals rely on Dilatation and Curettage for induced abortion and to treat post abortion complications, regardless of its invasiveness and comparatively high level of medical risk (Sathar et al, 2013).
Proposed strategy for action
In 2008, the International Federation of Gynecology and Obstetrics (FIGO) in collaboration with several stakeholders, including the International Confederation of Midwives (ICM), the United Nations of Population Fund (UNFPA), the WHO, Ipa and other local partners, launched an eight-year campaign for the prevention of unsafe abortions and its consequences which lasted till 2016. In total, 53 countries participated in the global campaign in which Pakistan was also one of the signatories. The campaign implemented a four-level comprehensive interventions package at country and regional levels. This included primary, secondary, tertiary and quaternary levels of prevention. The primary level included prevention of unintended pregnancies through promotion of family planning awareness and services, at large. The purpose of the secondary level prevention was to prevent unsafe abortions and to provide safe abortion services, where legal. The tertiary level prevention was based on provision of safe post-abortion services in conditions where women encountered unsafe abortion. The quaternary prevention was meant to prevent unsafe abortions in the future by promoting post-abortion family planning services. This campaign showed successful outcomes; as a result, provision of post-abortion care (PAC) and postpartum family planning have started gaining attention in Pakistan (Faundes et al, 2020).
Based on the FIGO's four levels of intervention for addressing unsafe abortions, the proposed comprehensive strategy (Figure 1) for actions at the individual, facility, community and policy levels can address the challenge of unsafe abortions in Pakistan.
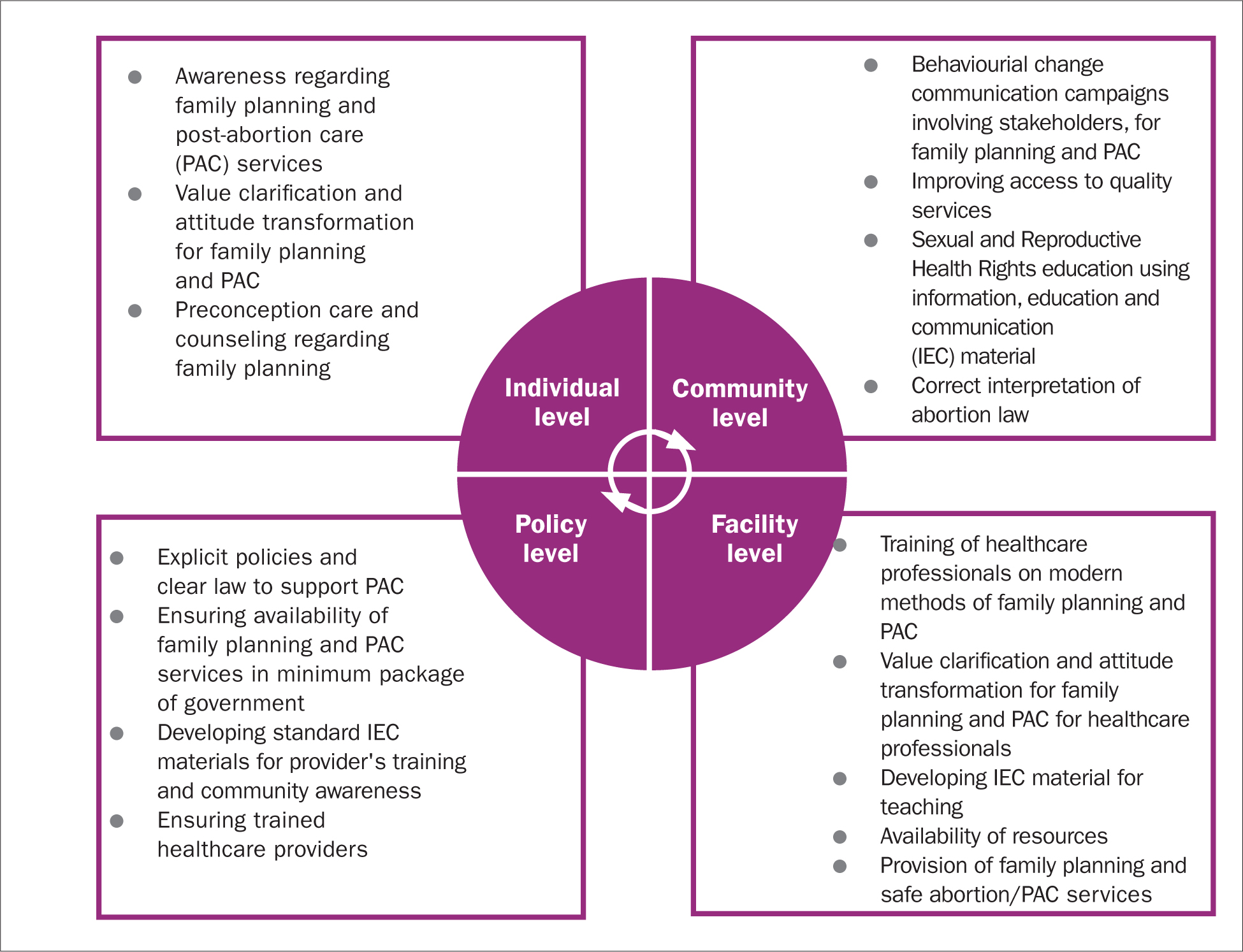 Figure 1. Comprehensive strategy to overcome unintended pregnancies and unsafe abortions
Figure 1. Comprehensive strategy to overcome unintended pregnancies and unsafe abortions
At the individual level, there is a need to conduct value clarification and attitude transformation (VCAT) sessions to spread awareness among adolescents, women of reproductive age, married women and their partners. Youth need to be engaged in preconception care and counseling, as indicated in the Sexual and Reproductive Health Rights (SRHR) package (UNFPA, 2019). VCAT sessions have also played a significant role in addressing issues and concerns of healthcare professionals, and have provided a platform for addressing their personal and professional values, conflicts and their resolution.
At the community level, behavioural change management campaigns should be initiated to engage key community leaders, such as religious scholars, male members and other significant family members, for increasing their awareness regarding the consequences of unintended pregnancies and unsafe abortions. Networking of healthcare professionals who are based in the community, providing SRH services should be encouraged and connected with nearby health facilities to ensure timely referrals. Mass media campaigns, including mobile health messages on phones can be initiated to create awareness to promote family planning and PAC services.
At the facility level, preparation of healthcare providers, including mid-level providers, for the provision of modern methods of family planning and post-abortion care, including manual vacuum aspiration and misoprostol, should be promoted through competency based capacity building trainings. To transform the negative attitude of healthcare providers about family planning and PAC, VCAT workshops should be conducted. Their empathetic communication with the family, especially with the women, can play a key role in preventing unsafe abortion practices that prevail in the community. Availability of constant supplies and resources for the provision of family planning and PAC services in the facilities should be ensured. In addition, it is important to ensure that the services that are legal in the country are of quality and are accessible to the women.
At the policy level, the government should introduce flexible and explicit policies for convenient implementation at different levels of care. This should also include protection of healthcare providers who are involved in providing family planning and post-abortion care services at the community level. Under the influence of the International Conference on Population and Development, Pakistan's law has also evolved and has become conducive for safe abortion to preserve maternal health and to provide necessary treatment (Zaidi et al, 2014). Moreover, the government should also ensure provision of standard information, education and communication (IEC) material for use in the training of community health workers and frontline healthcare providers working in hospitals and community settings. These resources can also be used to educate women about the dangers of unsafe abortions for themselves, their families and their communities, as a whole.
Conclusion
In Pakistan, low use of contraceptives, leading to high rates of unintended pregnancies, is the key factor behind increased numbers of induced abortions. Moreover, in countries like Pakistan, several other factors, such as lack of availability of quality services, financial barriers, stigma associated with abortion, and lack of awareness about abortion law, may lead to unsafe abortions. Hence, comprehensive multi-level strategies targeted at the individual, community, facility and policy level are proposed to prevent unintended pregnancies and to promote safe PAC services.
There is an urgent need to invest in family planning and PAC services in Pakistan through the health system strengthening approach. This includes enhancing the competencies of frontline health workers to provide quality family planning and PAC services, accessibility to quality services, including availability of constant supply of resources, and mass-level behavioural change communication activities using IEC material at the community level. Community centered, evidence-based researches are needed to uncover the ground realities. With the community based participatory approach, we can bring issues to the surface, intervene to break the vicious cycle, and implement strategies for positive outcomes.
Key points
- It is important to acknowledge that unintended pregnancies and unsafe abortion is one of the preventable contributors of maternal mortalities in Pakistan
- Understanding the underlying factors of unsafe abortion related to individual, facility, community and policy is crucial to customise the care, meeting the needs of the women
- A comprehensive package of interventions targeting primary, secondary, tertiary and quaternary levels of the health system are proposed to promote family planning and post-abortion care for addressing the issue at the country level
CPD reflective questions
- What are the opportunities for adolescent population in the country to be aware and get sensitised regarding the safe sexual and reproductive health practices and available services as per their needs and rights?
- Is the curriculum of frontline healthcare providers appropriately developing their knowledge, attitude and skills to deliver need-based family planning and post-abortion care services?
- How can the healthcare system contribute to transforming positive attitudes and behaviours of healthcare providers and public, regarding family planning and post-abortion care services?