
In February 2015, the National Institute for Health and Care Excellence (NICE, 2015) revised its ‘Diabetes in pregnancy’ guideline to include new recommendations based on evidence from recent clinical studies. This article will discuss aspects of the new guidance and its supporting evidence. In 2014, there were 695 233 live births in England and Wales (Office for National Statistics, 2015). It is estimated that up to 5% of all pregnancies are complicated with either pre-existing diabetes or gestational diabetes mellitus (GDM) (Confidential Enquiry into Maternal and Child Health (CEMACH), 2005), therefore affecting approximately 34 000 women per year.
Diabetes is one of the most common complications of pregnancy and encompasses both GDM diagnosed during pregnancy, pre-existing type 1 diabetes mellitus (T1DM), type 2 diabetes mellitus (T2DM) and other rare specific types of diabetes (American Diabetes Association, 2010).
The prevalence of T1DM and T2DM is increasing. In particular, T2DM is increasing in specific minority ethnic groups including people of African, Black Caribbean, South Asian and Middle Eastern family origin (CEMACH, 2005). Approximately 87.5% of pregnancies complicated by diabetes are estimated to be due to GDM, with 7.5% being due to T1DM and the remaining 5% to T2DM (NICE, 2015).
As a result of the landmark HAPO (hyperglycaemia and adverse pregnancy outcomes) study (HAPO Study Cooperative Research Group, 2002), a new consensus on the definition of GDM was adopted by the World Health Organization (WHO, 2013). Changes to the oral glucose tolerance test (OGTT) diagnostic criteria will result in many more women being diagnosed with GDM (NICE, 2015).
In December 2014, MBRRACE-UK published Saving Lives, Improving Mothers' Care (Knight et al, 2014), which highlighted the need for improvement in the care of women with pre-existing medical conditions. Nearly three quarters of women who died during pregnancy between 2009–2012 had a coexisting medical condition, which in 3.4% of cases was diabetes. Within this time period, three women died as a direct result of their diabetes (2.8%). Detailed review of these deaths indicated that all women had poor glycaemic control prior to conception and during their pregnancy.
What is gestational diabetes?
Throughout pregnancy, the placenta acts as an endocrine organ producing numerous hormones including oestrogen, cortisol and human placental lactogen (HPL). These hormones inhibit the function of insulin, thereby causing a rise in the mother's blood glucose levels. The resultant increase in blood glucose commonly occurs in the second (13–28 weeks) and third (29–40 weeks) trimesters, when placental hormones are produced in excess. With increasing insulin resistance, the pancreas is stimulated to produce increasing levels of insulin. When the pancreas cannot meet the increased insulin demand, this results in GDM.
In the HAPO study (HAPO Study Cooperative Research Group, 2002), a global population of approximately 25 000 non-diabetic women were studied. A continuous relationship between glycaemia and adverse pregnancy outcome was demonstrated. The adverse pregnancy outcomes reported included primary caesarean section and high birth weight. A greater association was found between maternal glucose levels at 24–32 weeks' gestation and frequency of adverse perinatal outcomes. More recently, the International Association of the Diabetes and Pregnancy Study Group has further analysed the HAPO study data and recommended revised diagnostic criteria for GDM (International Association of Diabetes and Pregnancy Study Groups Consensus Panel, 2010), which is reflected in the new NICE guidance on management of diabetes in pregnancy. If a diagnosis of GDM is confirmed, NICE (2015) recommends a review with the joint diabetes and antenatal clinic within 1 week.
Type 1 and 2 diabetes
Women with pre-existing T1DM and T2DM have an increased risk of adverse pregnancy outcomes, including miscarriage, fetal congenital anomalies and perinatal death. Table 1 lists contributory factors that are associated with adverse pregnancy outcomes.
| Unplanned pregnancy |
| Lack of preconception counselling |
| Maternal social deprivation |
| Smoking |
| Alcohol use |
| No contraceptive use 12 months prior to pregnancy |
| No preconception folic acid |
| Suboptimal glycaemic control prior to and during pregnancy |
| Pre-existing diabetic complications |
| Evidence of intrauterine growth restriction |
| Lack of retinal screening 12 months prior to pregnancy |
Preconception counselling
Preconception counselling should be provided by clinicians experienced in managing diabetes in pregnancy, and is a key priority for implementation identified in the updated NICE (2015) guidance. It is, arguably, one of the most significant features of managing women with diabetes and seeks to provide women with the knowledge and tools to empower them to optimise their own health, while reducing adverse pregnancy outcomes for both mother and baby.
Detailed information should be given to women about how their diabetes can affect pregnancy but also how the pregnancy may alter the control of their diabetes. It is important to discuss the role of diet, body mass index (BMI) and exercise. There is an increased risk of hypoglycaemia and impaired awareness of hypoglycaemia during pregnancy (Ringholm et al, 2012). Nausea and vomiting can affect blood glucose control, and the higher risk of having a baby who is large for gestational age (LGA) can increase the likelihood of birth trauma, induction of labour and caesarean section.
It is important that the health professional obtains a detailed clinical history establishing the woman's current understanding of her condition, medication history, and the presence and extent of any diabetes-related complications including neuropathy, nephropathy and retinopathy. Additionally, information should be sought about general diabetic control and monitoring, identification and management of hypoglycaemic episodes, admissions to hospital and any other comorbidities.
Health professionals should discuss all possible maternal and fetal complications and risks related to pregnancy and delivery. Good communication is needed to emphasise the relationship between adverse perinatal outcomes and the degree of maternal glycaemic control.
General pregnancy advice
There have been four main studies around the target range for blood glucose during pregnancy (Vääräsmäki et al, 2000; Ekbom et al, 2008; Mikkelsen et al, 2011; Barnes et al, 2013). Two of these studies (Mikkelsen et al, 2011; Barnes et al, 2013) suggest that a threshold of 37–38 mmol/mol reduced the incidence of LGA babies; however, there was no demonstrated reduction in the incidence of shoulder dystocia.
If an initial preconception consultation reveals poorly controlled diabetes—HbA1C >86 mmol/mol (10%)—avoidance of pregnancy should be clearly stipulated. This should be reinforced by discussion of current contraception methods and advice given accordingly. Any follow-up should be arranged to monitor glycaemic control and provide ongoing education and advice as to when is safe to start a family. It is important to provide education in a supportive environment and in language and literature that is appropriate to the woman's level of understanding. Attendance of partners and/or family members should be encouraged where possible.
Women require practical and tailored information about their diet and nutrition. If enquiry into dietary routines reveals poor habits and nutritional balance, referral to a dietician is indicated (Ray et al, 2001).
Information leaflets and signposting to websites for further information can help to educate women and provide continuous support at home. Particularly important to women with pre-existing diabetes is an understanding of foods with a low glycaemic index as these result in a slower and steadier release of glucose. Any myths regarding ‘eating for two’ or the need for full-fat milk should be dispelled. Midwives should explain to women that energy requirements in the first 6 months of pregnancy do not change, and in the remaining 3 months only increase slightly (by 200 calories per day, assuming energy intake is not already exceeding the recommended daily intake) (NICE, 2010a).
All women with pre-existing diabetes should supplement their diet with a daily dose of 5 mg folic acid 3 months prior to conception, and continue this until at least 12 weeks gestation, to reduce the risk of neural tube defects (Capel and Corcoy, 2007).
If the woman smokes, signposting to local smoking cessation support services is essential to improve overall cardiovascular health and the additional risks posed to the pregnancy.
Women should aim to engage in exercise of moderate intensity for at least 30 minutes a day. This is not considered harmful to the baby and, indeed, has many benefits to the mother and pregnancy. If women are new to exercise, they should initially start with 15-minute sessions three times a week, and gradually build this up. Promotion of a more active lifestyle reduces the risks of venous thromboembolism and can contribute to healthy weight maintenance together with physical and emotional wellbeing (Harris and White, 2005).
Maternal complications
Women with diabetes present several medical risks when pregnant. Clinicians need to consider both how the diabetes affects development of other medical problems such as pre-eclampsia and infections, as well as how pregnancy alters the diabetic disease process and glycaemic control (Table 2).
| Effect of pregnancy on pre-existing diabetes | Effect of pre-existing diabetes on pregnancy | Obstetric problems increased in women with diabetes |
|---|---|---|
| Increasing insulin requirements and changes to glycaemic control | Increased risk of miscarriage | Polyhydramnios |
| Increasing episodes of hypoglycaemia | Increased risk of pre-eclampsia | Shoulder dystocia |
| Hypoglycaemic unawareness | Increased risk of infections—urinary tract, respiratory, endometrial, wound infections | Instrumental delivery |
| Vaginal candidiasis is very common | Induction of labour | Caesarean section |
| Deterioration in nephropathy especially with regards to proteinuria | Worsening renal function can result in severe oedema and a normocytic anaemia | Postpartum haemorrhage |
| Progression of diabetic retinopathy or new onset retinopathy | ||
| Ketoacidosis |
Women with diabetes who are pregnant have a three-to fourfold increased risk of pre-eclampsia, which is further worsened if there is evidence of pre-existing hypertension or renal disease. This risk directly relates to glycaemic control at conception and in early pregnancy, whereby each 1% fall in HbA1C below 20 weeks' gestation reduces the risk by 40% (Nelson-Piercy, 2010). Studies have shown that a daily dose of 75 mg of aspirin can reduce the occurrence of pre-eclampsia. All women with diabetes are therefore advised to take aspirin daily from 12 weeks until delivery (NICE, 2010b).
Retinal assessment during pregnancy
The Diabetes Prevention Program Research Group (2007) cohort study determined the prevalence of retinopathy characteristically seen in people with diabetes. The study found that pregnancy is independently associated with the progression of diabetic retinopathy. The increased risk may be due to suboptimal control itself, or to the rapid improvement in metabolic control that may have occurred in early pregnancy.
Therefore, all women with pre-existing diabetes who are planning a pregnancy, or find themselves pregnant, should have a retinal screen during the first trimester of pregnancy (unless they have already been screened within the last 3 months). They should also have a repeat retinopathy screen at 28 weeks.
Diabetic retinopathy should not be considered a contraindication to rapid optimisation of blood glucose control in women who present with a high HbA1c in early pregnancy. The Diabetes Control and Complications Trial (1993) demonstrated that, overall, people with early worsening of retinopathy who intensively improve their glucose control reduce the risk of subsequent progression compared with people who do not optimise control. Health professionals should ensure that women who have pre-proliferative diabetic retinopathy, or any form of referable retinopathy diagnosed during pregnancy, have ophthalmological follow-up for at least 6 months after the birth of the baby. Diabetic retinopathy should not be considered a contraindication to vaginal birth. This recommendation is reflected in the updated NICE (2015) guidance.
Renal assessment during pregnancy
The systematic review by Rosenn and Miodovnik (2003) included 11 studies involving a total of 201 people. The overall conclusion from most studies suggested that pregnancy is not associated with the development of nephropathy or accelerated progression of pre-existing nephropathy. The exception to this is in women with moderate to advanced disease, where pregnancy may accelerate to end-stage renal disease. Women with diabetic nephropathy have further increased risks of adverse pregnancy outcomes, in particular fetal growth restriction, hypertension, pre-eclampsia and preterm birth (NICE, 2015).
Glycaemic control during pregnancy
In early pregnancy, poor glycaemic control can result in dysfunctional embryogenesis leading to early pregnancy loss (miscarriage) or fetal abnormalities.
Increased insulin resistance during pregnancy ultimately interferes with glycaemic control. Women will observe increasing insulin requirements to maintain euglycaemia and are likely to experience increasing hypoglycaemic episodes. Reduced identification of these episodes—so-called ‘hypoglycaemia unawareness’—is common in pregnancy and can be dangerous to the mother. Hypoglycaemia remains the leading cause of maternal deaths among diabetic women and it is therefore crucial for mothers to increase glucose monitoring and have regular specialist review.
Following on from the HAPO study (HAPO Study Cooperative Research Group, 2002), NICE amended its guidance around target blood glucose levels and suggested agreed individualised targets for self-monitoring of blood glucose with women both with GDM and those with pre-existing diabetes, taking into account the risk of hypoglycaemia. These targets should be aimed to be achieved without causing problematic hypoglycaemia of a fasting level of 5.3 mmol/l and a 1-hour post-meal of 7.8 mmol/l or a 2-hour post-meal of 6.4 mmol/l. All those women treated with insulin or a sulphonylurea should aim to maintain their blood glucose level above 4 mmol/l.
Fetal complications
The majority of fetal and newborn complications associated with diabetes are a direct result of hyperglycaemia. A study by Fraser (2011) showed that women with diabetes are at increased risk of having babies with congenital abnormalities and this is directly correlated with HbA1C around conception. Women with HbA1C <69 mmol/mol (8%) have a risk of approximately 5% compared to HbA1C >86 mmol/mol (10%) with a risk as high as 25% (Nelson-Piercy, 2010).
Congenital anomalies that are more common in pregnancies complicated by diabetes include cardiac, neurospinal, gastrointestinal, musculo-skeletal, renal and cleft lip and palate.
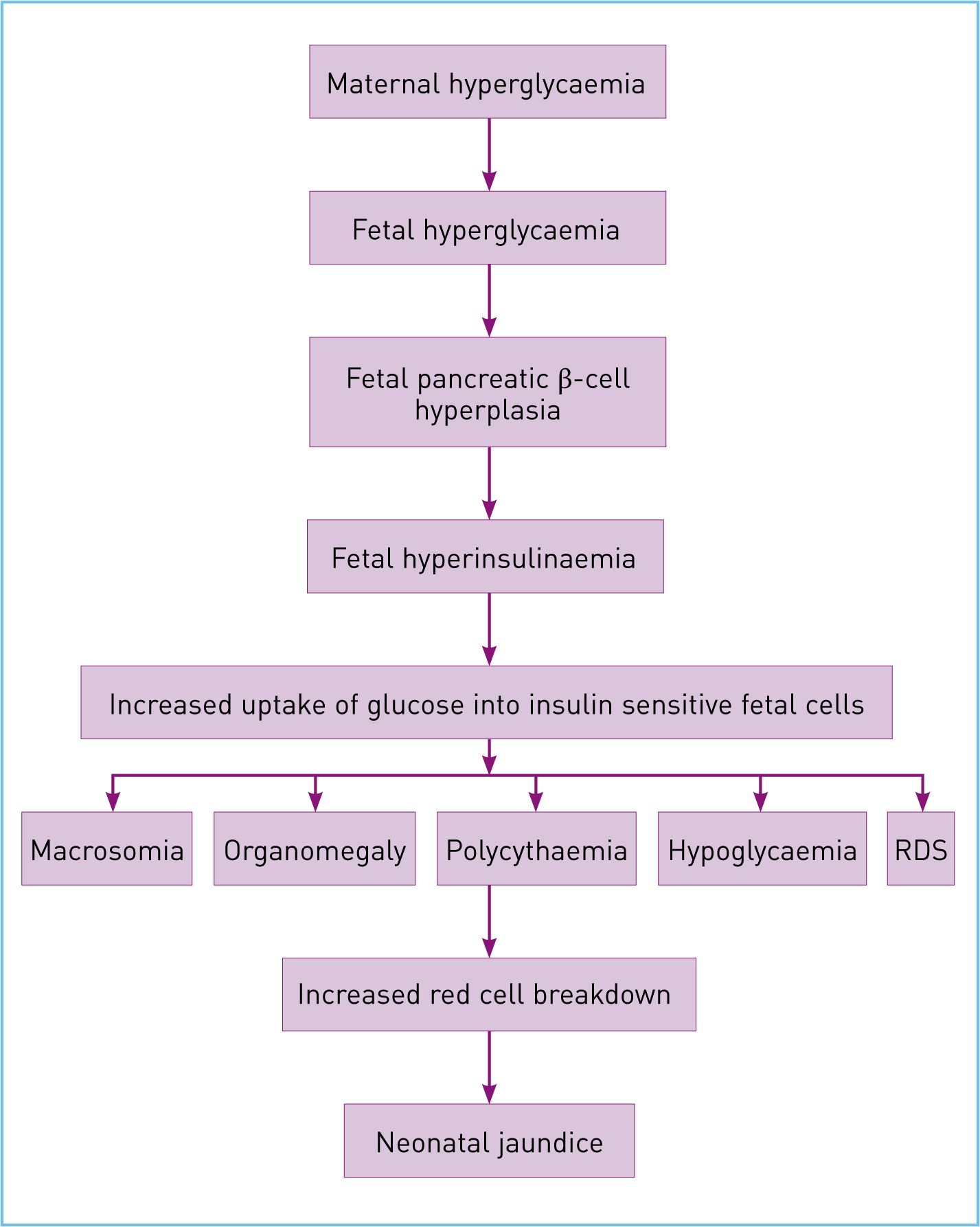
Apart from congenital malformations, babies of women with diabetes are at increased risk of late stillbirth, neonatal mortality, macrosomia, preterm birth (partly iatrogenic), neonatal hypoglycaemia, polycythaemia, jaundice and respiratory distress syndrome. The proposed pathogenesis of these complications is illustrated by the Pederson hypothesis (Figure 1).
It is important to realise that late intrauterine deaths cannot be predicted from cardiotocograph, Doppler velocimetry or biophysical profiles. This is, therefore, an important justification for recommending early induction of labour or elective caesarean section between 37+0 and 38+6 weeks gestation in these women. Continuous electronic fetal monitoring in labour is recommended (NICE, 2015).
To help identify fetal macrosomia and to monitor growth, women with diabetes should have serial ultrasound scans throughout their pregnancy. This helps dictate ongoing management and decisions about timing delivery (Royal College of Obstetricians and Gynaecologists, 2013).
The role of the multidisciplinary team
NICE (2015) considered the benefits of multidisciplinary teams (MDTs) and, when comparing women receiving care from a MDT with women receiving standard care, glycaemic control was better in the group of women receiving care from a MDT. For fetal outcomes, there were significantly fewer miscarriages and significantly fewer specialist care baby unit admissions in this group of women. Therefore, it is recommended that all women with pre-existing diabetes or GDM should be offered immediate contact with a joint diabetic antenatal clinic. They should also have contact with the clinic for assessment of their blood glucose control every 1–2 weeks throughout the pregnancy.
Conclusion
Owing to the evidence that predisposes women with diabetes to be considered at a greater risk during pregnancy, most are willing to play their part in trying to achieve a successful outcome. A multidisciplinary team approach in tandem with the woman and her family can improve glycaemic control. Careful monitoring and ongoing education aims to assist in the provision of a positive, balanced management plan, which is integral to achieving successful perinatal outcomes and maintaining maternal health.