
Postnatal depression is a significant global health issue and affects 26–85% of postpartum women who experience the so-called ‘baby blues’. Of these, 10–15% have been found to deteriorate to a major depressive disorder (Epperson and Ballew, 2008). In the UK, it is estimated that 1 in every 10 women are affected by postnatal depression (NHS Choices, 2016), while in Australia and the USA the estimate is as high as 1 in 5 women (Australian Institute of Health and Welfare, 2012; Centers for Disease Control and Prevention, 2017). Postnatal depression often presents with a greater incidence with a comorbid anxiety or may develop into bipolar affective disorder (Munk-Olsen et al, 2012). Postpartum psychosis is another comorbidity that may co-occur in 0.1–0.2% of all new postnatal women (Kendall-Tackett, 2010). Suicide occurs in some severe cases of postnatal depression and in Australia, New Zealand and the UK has been identified as the most common yet most preventable cause of maternal death (Knight et al, 2017; Australian Institute of Health and Welfare, 2017; Perinatal and Maternal Mortality Review Committee, 2017). In the UK, £8.1 billion is spent on perinatal mental health each year (Bauer et al, 2014) and it is considered a priority for health policy (Royal College of Obstetricians and Gynaecologists, 2017).
The specific pathophysiology of postnatal depression is thought to be due to the rapid hormonal changes taking place across the perinatal period (Brummelte and Galea, 2016), with an overall prevalence of 13% within the first 12 weeks following birth (O'Hara and Swain, 1996). The physiological stress, combined with the multifaceted psychosocial stressors of pregnancy, place the predisposed individual, or those less resilient, at risk.
The effects of postnatal depression can be alarming. Some studies have indicated that mothers with postnatal depression may experience poor interaction and bonding with their child and that there is a risk of cognitive impairment of the child (Brummelte and Galea, 2016).
Western medical treatments include antidepressants and psychological and psychosocial interventions, including cognitive behaviour therapy and mindfulnessbased therapy. Alternative therapies are also sought that include omega-3 fatty acids, hormone therapy, electroconvulsive therapy and bright light therapy (Fitelson et al, 2010).
The effectiveness of psychological and psychosocial interventions is supported in the evidence, while there is insufficient evidence for other forms of management (Fitelson et al, 2010; Molyneaux et al, 2014). Antidepressants carry known and unknown risks for breastfeeding infants and present potential negative effects on the child's development. They are therefore not a preferable treatment option for many women (Lanza Di Scalea and Wisner, 2009; Fitelson et al, 2010; Guille et al, 2013; Ornoy and Koren, 2014).
In Korea, Japan and China, after birth, families encourage traditional approaches, such as prescribing the mother with a period of rest and intensive family support during the postpartum period (Fok et al, 2016). Another approach often adopted in Asian countries is traditional Chinese medicine, which consists primarily of acupuncture and/or herbal medicine. The treatment of postnatal depression is based on principles of syndrome differentiation. The two key sub-types are deficiency of qi (a circulating life force) and blood, and zang organs (Betts, 2005; West, 2008; Clavey, 2013; Xi et al, 2015).
Within traditional Chinese medicine, there is growing interest in the use of acupuncture for depression in particular, with a growing body of evidence to support the benefits of acupuncture for depression in adults (Smith et al, 2018) as well as studies showing acupuncture achieving similar effects to medication in the management of depression across the perinatal period (Manber et al, 2010; Xu et al, 2013) In addition, acupuncture is safe (Zhang et al, 2010; Mcdonald and Janz, 2017) and may also be cost effective in comparison to conventional care or psychological interventions (Spackman et al, 2014). This emerging evidence has boosted the popularity of acupuncture for treating depression in the US (Clarke et al, 2015; Borah et al, 2017) and the UK, where it is particularly sought after by women (Hopton et al, 2012).
However, despite the increasing demand for the use of acupuncture for depression there has yet to be a systematic review that specifically provides an overview of the evidence for using acupuncture in the management of postnatal depression.
Objectives
This study aims to systematically review the literature to evaluate the effectiveness and safety of acupuncture for postnatal depression, when compared with standard psychopharmacologic antidepressant treatment.
Antidepressant therapy is widely used for postnatal depression and is often the first-line option for women who are experiencing moderate-to-severe depression, and who are not offered or cannot access psychological or psychosocial interventions (Molyneaux et al, 2014). Determining the effectiveness of acupuncture compared to antidepressants may lead to acupuncture being used to complement, or act as an alternative to, antidepressants.
Methods
Search strategy
Guided by the Cochrane Handbook of Systematic Review of Interventions (Higgins and Green, 2011), electronic searches were conducted in a range of international databases, without language restrictions:
All databases were searched from their inception to June 2018. A broad range of search terms were included, related to perinatal depression and to acupuncture therapies such as moxibustion. A combination of terms and synonyms were used, including acupuncture, electroacupuncture, auricular acupuncture, scalp acupuncture, laser acupuncture, moxibustion, acupressure, dry needling; prenatal depression, antenatal depression, postnatal depression, postpartum depression, puerperal depression, perinatal depression and randomised controlled clinical trial. Search terms were translated and modified accordingly to suit the Chinese, Korean and Japanese databases.
Terms relating to specific antidepressants were excluded from the database search, as there are various classes of antidepressants and those commonly used vary between countries. Basing the search on the types of oral antidepressants used in those studies may have limited the search and increased the risk of missing otherwise relevant literature.
Study selection criteria
Inclusion criteria were published randomised controlled trials in any language; diagnosis of depression according to standard diagnostic criteria such as the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) (American Psychiatric Association Task Force on DSM-IV, 2000) or 5th Edition (American Psychiatric Association, 2013), the International Classification of Disease-10 Classification of Mental and Behavioral Disorders (World Health Organization, 1992) and the third version of the Chinese Classifications of Mental Disorders (CCMD-3) (Chen, 2002); women in the perinatal period; studies comparing acupuncture or acupuncture-related therapies against any oral antidepressants; severity of disease measured by a standardised outcome measure of depression. Occurrence of adverse events; safety profiles; birth data such as gestation, Apgar score, infant weight, quality of life and mode of birth (vaginal or caesarean section); and participant/acupuncturist expectations were evaluated as secondary outcome measures, if such data were available. Strict selection criteria were adhered to in an attempt to minimise heterogeneity among included studies, thereby increasing the clinical applicability.
Data extraction and quality assessment
Database searches and article screening were independently conducted by three authors (AK, DA and SR) for the English databases; two authors (HYT and RU) for the Japanese databases; and one author for the Chinese (LZ) databases and Korean databases (MA), respectively.
Details of the trial design, participants, sample size, intervention, methodological quality and outcome measures were extracted into an Excel sheet by one author for each language and data was checked by at least one other author. Assessment of risk of bias and assessment of quality of reporting was conducted by two independent assessors based on the Cochrane Collaboration tool for assessing risk of bias (Higgins et al, 2011) and the Standards for Reporting Interventions in Clinical Trials in Acupuncture (STRICTA) (MacPherson et al, 2010; 2015). There were disagreements on study selection, which were resolved through discussion with a third assessor (ZZ). There were no disagreements on data extraction and assessment of risk of bias.
Data analysis
Data from relevant outcome measures were entered and analysed using the Cochrane Review Manager 5.3. Only published data were included in the analysis. Dichotomous data were presented as risk ratio, while for studies using the same outcome measures, continuous outcomes were reported as mean difference with 95% confidence intervals. Heterogeneity was calculated using the tau-squared (t2), iota-squared (I2), chi-squared (χ2) statistical methods; heterogeneity was considered substantial when t2>0, with a combination of either an I2 value of more than 50% or a P-value with a χ2 test score of less than 0.10. A random-effects model was used if there was significant heterogeneity (I2≥ 50%), while a fixed-effects model was used when heterogeneity was less than 50% (I2≤ 50%) (Higgins and Green, 2011).
Results
Description of studies
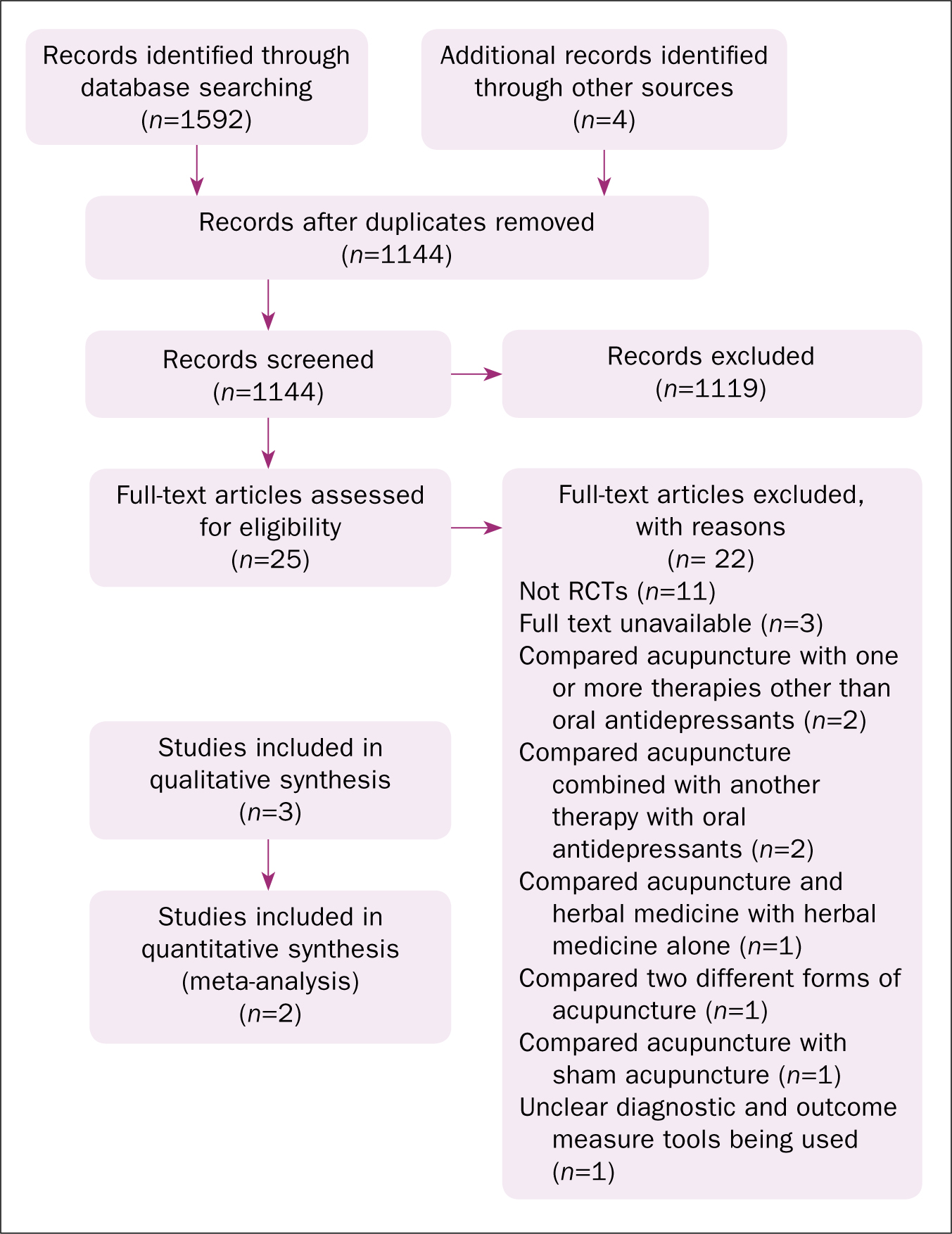
The electronic search revealed 1592 studies. After screening of titles and abstracts, duplicates and irrelevant hits were excluded for the reasons shown in Figure 1. Three studies met the inclusion criteria for quantitative analysis (Chen et al, 2010; Dong and Gao, 2014; Yu et al, 2015). Due to insufficient reporting of data from the Hamilton Rating Scale for Depression (HRSD), the Dang and Gao (2014) study was excluded, leaving two studies (Chen et al, 2010; Yu et al, 2015), involving a total of 112 participants included in the meta-analysis. The electronic study selection strategy is pictorially represented in the PRIMSA reporting guideline diagram (Moher et al, 2009) (Figure 1).
All three studies were conducted in China and compared acupuncture with the oral antidepressant fluoxetine. All participants were women above the age of 18 years, without previous diagnosis of other psychiatric disorders such as schizophrenia or bipolar disorder, or other serious physical illness. Diagnosis of depression was based on the criteria of the CCMD-3 in postpartum women, with no mention of time of onset after birth. All three studies adopted the HRSD as the primary outcome measure; one study (Yu et al, 2015) evaluated quality of life using the 36-Item Short Form Health Survey (SF-36); two studies evaluated the occurrence of adverse events (Chen et al, 2010; Yu et al, 2015). Interestingly, none of the studies used the Edinburgh Postnatal Depression Scale (EPDS).
Assessment of risk of bias
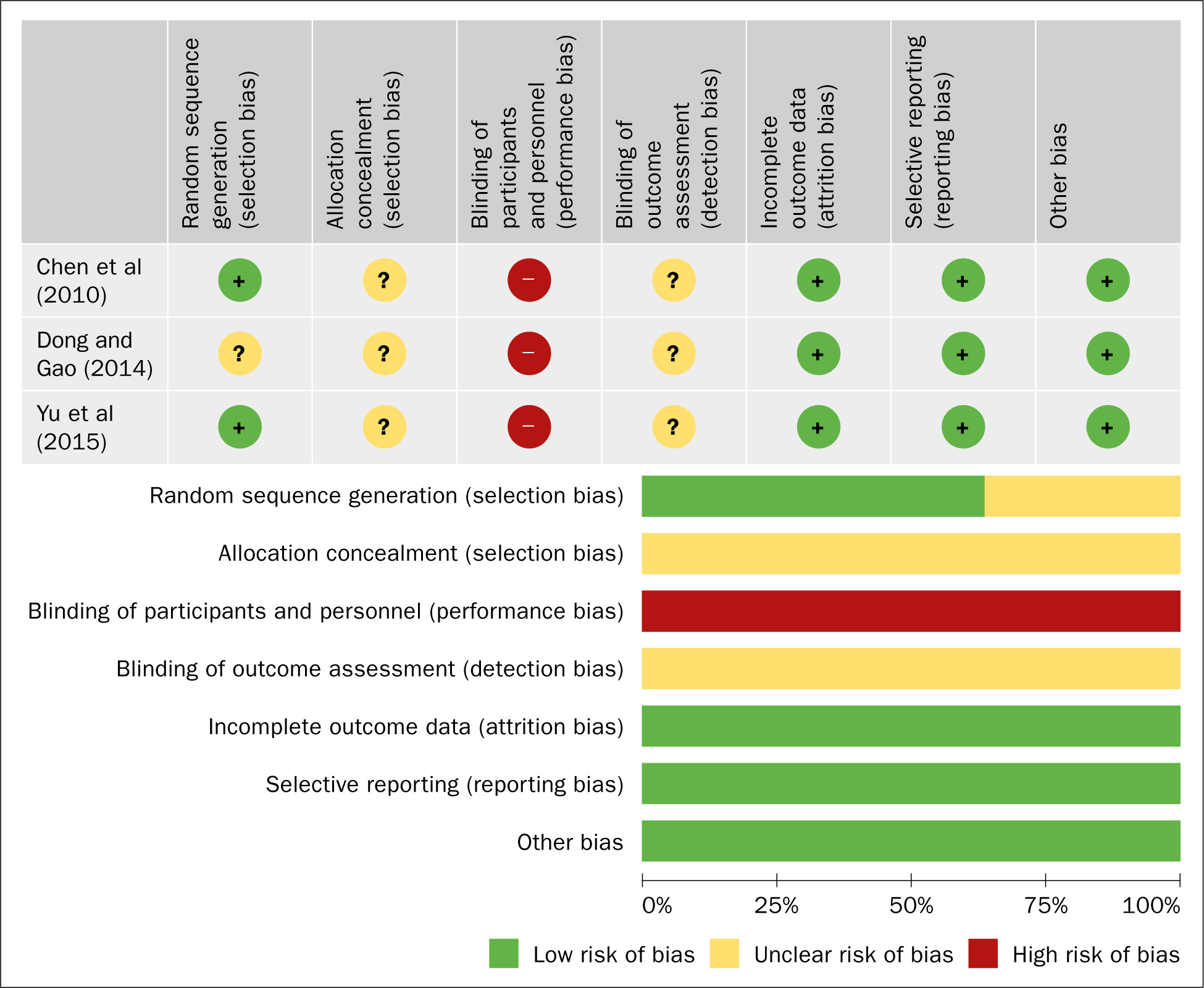
The criteria for assessment of risk of bias included random sequence generation, allocation concealment, blinding and incomplete outcome data. Selective reporting could not be assessed as none of the studies had a published protocol nor had been registered before publication. Two studies (Chen et al, 2010; Yu et al, 2015) mentioned using a random table of numbers and were judged with low risk for sequence generation; none of the studies mentioned allocation concealment and were judged with unknown risk. Blinding of participant and treatment personnel was not possible due to the different forms of treatment modalities between groups; however, none of the studies mentioned whether outcome assessors were blinded and were therefore judged with high risk of detection bias. There were no drop-outs in any of the three studies; therefore, there was a low risk of attrition bias (Figure 2).
STRICTA assessment
STRICTA is a reporting system that is designed for assisting authors to present their acupuncture trial in an accurate, transparent, and complete manner in order to facilitate clear interpretation and replicability (MacPherson et al, 2015). As presented in Tables 1 and 2, all studies clearly described the acupuncture points used; however, none offered explanations of practitioner background and some details of needling were lacking. Two studies reported that the needling sensation, de qi, was sought and all three studies clearly stated stimulation methods employed. Frequency and duration of treatment ranged from 5 times per week for 6 weeks (Chen et al, 2010), 5 times per week for 4 weeks (Yu et al, 2015), to 30 consecutive daily treatments (Dong and Gao, 2014).
| Source | Sample size | Age group (years) | Diagnostic criteria; disease severity | Treatment Intervention | Control intervention | Outcome measure (s) | ||
|---|---|---|---|---|---|---|---|---|
| Style of acupuncture | Acupuncture points | Stimulation/retention | ||||||
| Chen et al (2010) |
n=52 |
T=24–34 (mean=27.8) |
CCMD-3 |
Acupuncture | Baihui (GV 20); |
Even method stimulation was performed until a comfor table distension of the local region was felt. Needles were retained for 30 minutes. Treatment 5 times a week for 6 weeks | Orally administered fluoxetine hydrochloride, 20mg, once per day for 6 weeks | HRSD score and reduction in HRSD (%) |
| Dong and Gao (2014) |
n=60 |
22–34 (mean=26.7) | CCMD-3 |
Threading scalp acupuncture Standard acupuncture | Xuanlu (GB5) through Xuanli (GB6); |
For threading scalp acupuncture, each needle was stimulated for 1 minute and retained for 40 minutes. For standard acupuncture, each needle was stimulated using rotation/lifting and thrusting method after de qi was achieved, and then retained for 40 minutes. Treatment once a day for 30 days | Orally administered fluoxetine hydrochloride, 20mg, once per day for 1 month | Reduction in HRSD (%) and score (score not repor ted) |
| Yu et al (2015) |
n=60 |
T=28± 16 |
CCMD-3 |
Standard acupuncture (Sun Si Miao's 13 ghost points) | Shuigou (GV 26); |
Even method stimulation was performed after de qi was achieved; needles retained for 30 minutes. Treatment once a day, five times a week, for 4 weeks | Orally administered fluoxetine hydrochloride capsules, 20mg, once per day for 4 weeks | HRSD score, SF-36 score |
T: treatment size; C: control; D: drop-out; CCMD-3: Chinese Classifications of Mental Disorders; HRSD: Hamilton Rating Scale for Depression
| Item | Detail | Chen et al (2010) | Dong and Gao (2014) | Yu et al (2015) |
|---|---|---|---|---|
| 1. Acupuncture rationale | 1a) Style of acupuncture (e.g. traditional Chinese medicine, Japanese, Korean, Western medical, Five Element, ear acupuncture, etc) | ˟ | ✓ | ✓ |
| 1b) Reasoning for treatment provided (based on historical context, literature sources, and/or consensus methods) with references where appropriate | ✓ | ✓ | ✓ | |
| 1c) Extent to which treatment was varied | ˟ | ˟ | ✓ | |
| 2. Details of needling | 2a) Number of needle insertions per subject per session (mean and range where relevant) | ✓ | ✓ | ✓ |
| 2b) Names (or location if no standard name) of points used (uni/bilateral) | ✓ | ✓ | ✓ | |
| 2c) Depth of insertion, based on a specified unit of measurement, or on a particular tissue level | ˟ | ✓ | ˟ | |
| 2d) Response sought (e.g. de qi or muscle twitch response) | ✓ | ✓ | ✓ | |
| 2e) Needle stimulation (e.g. manual, electrical) | ✓ | ✓ | ✓ | |
| 2f) Needle retention time | ✓ | ✓ | ✓ | |
| 2g) Needle type (diameter, length, and manufacturer or material) | ✓ | ˟ | ✓ | |
| 3. Treatment regimen | 3a) Number of treatment sessions | ✓ | ✓ | ✓ |
| 3b) Frequency and duration of treatment sessions | ✓ | ✓ | ✓ | |
| 4. Other components of treatment | 4a) Details of other interventions administered to the acupuncture group (e.g. moxibustion, cupping, herbs, exercises, lifestyle advice) | N/A | N/A | N/A |
| 4b) Setting and context of treatment, including instructions to practitioners, and information and explanations to patients | ˟ | ˟ | ˟ | |
| 5. Practitioner background | 5) Description of participating acupuncturists (qualification or professional affiliation, years in acupuncture practice, other relevant experience) | ˟ | ˟ | ˟ |
| 6. Control or comparator interventions | 6a) Rationale for the control or comparator in the context of the research question, with sources that justify this choice | ˟ | ˟ | ˟ |
| 6b) Precise description of the control or comparator. If sham acupuncture or any other type of acupuncture-like control is used, provide details as for items 1 to 3 above. | ✓ | ✓ | ✓ |
Primary outcome measures
Disease severity
The HRSD was the primary outcome measure in all three studies and is one of the earliest and most widely used scales for clinical studies of depression (Cusin et al, 2010). The total score of the 17 items, with a maximum possible of 52, indicates the presence and severity of the condition: 0-6 indicates no depression; 7-17 indicates mild depression; 18-24 indicates moderate depression; while scores above 24 indicate severe depression. A reduction of at least half the score from baseline is said to be a significant change (Cusin et al, 2010).
One study (Dong and Gao, 2014) did not report the HRSD scores and could not be included in the meta-analysis. The authors of the study reported that acupuncture had an effective rate of 86.7% compared to the effective rate of fluoxetine of 73.3%, with no indication if there was a significant difference.
Yu et al (2015) found that both acupuncture and fluoxetine were effective, with the outcomes in the acupuncture group significantly higher. However, this result differs from that of Chen et al (2010), who also found both therapies effective, but reported no significant differences between fluoxetine and acupuncture (Table 3). Furthermore, the meta-analysis (Table 4) comparing the combined data from both studies revealed no significant differences between the acupuncture and fluoxetine groups. A high level of heterogeneity (I2=84%; P=0.36) was apparent in the results of the meta-analysis, and may have stemmed from differences in acupuncture treatments, whereby completely different sets of acupuncture points were used in each study.
| Yu et al (2015) | Chen et al (2010) | |||
|---|---|---|---|---|
| Experimental | Control | Experimental | Control | |
| Baseline | 29.83 ± 2.97 | 28.90 ± 3.17 | 20.192 ± 2.078 | 20.346 ± 1.979 |
| After 2 weeks | 16.885 ± 1.986 | 17.346 ± 1.853 | ||
| After 4 weeks | 11.53 ± 5.87 | 16.50 ± 8.22 | 13.615 ± 2.368 | 14.154 ± 2.185 |
| After 6 weeks | 10.500 ± 2.902 | 10.538 ± 2.716 | ||
Yu et al (2015): Experimental group received acupuncture treatment once daily for 30 consecutive days, totaling 30 sessions. Control group received oral fluoxetine hydrochloride at 20 mg per day for 30 consecutive days.
Chen et al (2010): Experimental group received acupuncture treatment once a day, 5 times per week for 4 weeks, totaling 20 sessions. Control group received oral fluoxetine capsules at 20 mg per day for 4 weeks.
HRSD: Hamilton Rating Scale for Depression
| Experimental | Control | Mean Difference | Mean Difference | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Study or subgroup | Mean | SD | Total | Mean | SD | Total | Weight | IV, Random, 95% Cl | IV, Random, 95% Cl |
| Chen et al (2010) | 10.5 | 2.902 | 26 | 10.538 | 2.716 | 26 | 55.7% | -0.04 [1.57, 1.49] |
|
| Yu et al (2015) | 11.53 | 5.87 | 30 | 16.5 | 8.22 | 30 | 44.3% | -4.97 [-8.58, -1.36] | |
| Total (95% Cl) | 56 | 56 | 100.0% | -2.22 [-7.02, 2.58] | |||||
Heterogeneity: Tau2 = 10.16; Chi2 = 6.07, df = 1 (P=0.01); Iota2 = 84% Test for overall effect: Z = 0.91 (P=0.36)
HRSD: Hamilton Rating Scale for Depression
Secondary outcome measures
Quality of life
The SF-36 is a self-administered 36-item questionnaire that measures health based on eight dimensions: physical functioning, social functioning, role limitations, mental health, vitality, pain, general health perception and health change (Brazier et al, 1992).
One study (Yu et al, 2015) used the SF-36 questionnaire and reported that acupuncture performed significantly better than fluoxetine in several dimensions of the SF-36, including pain, general health, vitality, social functioning, mental health and health transition (Table 5).
| Experimental (acupuncture) | Control (fluoxetine) | |||
|---|---|---|---|---|
| Baseline | End of Tx | Baseline | End of Tx | |
| Physical functioning | 70.80 ± 22.96 | 89.01 ± 8.38 | 68.24 ± 21.77 | 76.49 ± 17.79 |
| Physical role functioning | 26.85 ± 37.45 | 82.10 ± 28.29 | 17.57 ± 31.11 | 59.46 ± 28.29 |
| Bodily pain | 55.48 ± 28.53 | 74.02 ± 18.74 | 54.27 ± 29.62 | 77.51 ± 23.03 |
| General health perceptions | 54.81 ± 23.88 | 74.85 ± 14.71 | 56.89 ± 19.66 | 57.43 ± 14.70 |
| Vitality | 54.17 ± 24.53 | 81.02 ± 16.43 | 59.80 ± 27.97 | 56.88 ± 17.84 |
| Social role functioning | 32.92 ± 42.33 | 90.57 ± 25.95 | 39.64 ± 47.03 | 72.97 ± 38.36 |
| Emotional role functioning | 56.00 ± 20.73 | 76.90 ± 14.46 | 64.43 ± 23.98 | 70.81 ± 8.16 |
| Mental health | 2.69 ± 0.76 | 3.91 ± 0.68 | 2.36 ± 0.49 | 3.41 ± 0.67 |
| Health transition | 38.46 ± 28.64 | 55.83 ± 14.00 | 38.43 ± 19.12 | 45.57 ± 11.61 |
Occurrence of adverse events
Yu et al (2015) reported that neither the acupuncture nor the fluoxetine group had any adverse events. Chen et al (2010) reported that there were no adverse events in the acupuncture group, but in the fluoxetine group, there were four cases of nausea, four cases of decreased appetite and two cases of dizziness.
Discussion
Only three studies, all originating in China, met the inclusion criteria for this review. Despite the high risk of bias and small sample sizes, each reported that acupuncture was effective in improving postnatal depression and comparable to the oral antidepressant, fluoxetine hydrochloride. One study reported that acupuncture performed significantly better in improving certain aspects of quality of life (Yu et al, 2015). The meta-analysis showed no significant difference between acupuncture and fluoxetine, which supports the hypothesis that acupuncture is equally as effective as fluoxetine in the management of postnatal depression. There was a high level of heterogeneity, which calls for further research to determine the best practice related to acupuncture technique and point selection, and evidence to guide frequency and length of treatment for treating postnatal depression.
There have been a number of previous reviews on acupuncture for depression, including an updated Cochrane review (Smith et al, 2018) and a systematic review of systematic reviews on the topic (Ernst et al, 2011). According to the latter study, there were mixed conclusions among the systematic reviews, with those originating in China or consisting primarily of studies from China being more likely to present positive data; two reviews showed that there were no significant differences in effectiveness between acupuncture and antidepressants (Zhang et al, 2010; Smith et al, 2018). There was also a general consensus in the reviews about the lack of high quality studies, which may affect the conclusions. It should be noted that none of the studies were focused specifically on postpartum women.
Acupuncture is said to help in the management of psychological conditions such as depression by stimulating the secretion of hormones such as serotonin and encephalin in the central nervous system and plasma (Cabýoglu et al, 2006). Another study showed that acupuncture inhibited the inflammatory response by modulating nuclear factor kappa B (NF-kB) in the brain, resulting in antidepressant-like effects (Lu et al, 2017). However, neither of these two studies mentioned acupuncture point specificity; that is, whether the choice of acupuncture points played a role in the results.
When considering the management of postnatal depression, one of the main concerns is safety. The most recent review on this topic (Mcdonald and Janz, 2017) considered acupuncture as an inherently safe treatment modality when administered by well-trained practitioners. They also found acupuncture a safe and well-tolerated treatment option for major depressive disorders (Mcdonald and Janz, 2017). Other systematic reviews on the safety of acupuncture during pregnancy, have concluded that adverse events are minor or small in number when the treatment is applied appropriately (Ernst and White, 2001; Park et al, 2014; Clarkson et al, 2015). There were no adverse events relating to acupuncture reported in the reviewed studies, supporting the view that acupuncture is safe and well tolerated.
Apart from being the first systematic review on acupuncture for postnatal depression, this article focused on an important question highly relevant to clinical practice: is there a safe and effective adjuvant or alternative management to antidepressant medication for postnatal depression? The previous Cochrane review on the effects of acupuncture for depression included multiple types of controlled interventions and showed no significant difference between verum acupuncture and sham acupuncture (Smith et al, 2018). Indeed, the discussion regarding the therapeutic or placebo effects of acupuncture compared to sham acupuncture is ongoing (Zhang et al, 2015) although there are studies that found different physiological responses were elicited when applying verum acupuncture compared to sham acupuncture (Enck et al, 2010). As the objective of this review was to evaluate the effectiveness, not the efficacy, of acupuncture, only studies specifically comparing acupuncture with the routine management of postnatal depression with oral antidepressants, were included. A comparison between acupuncture treatment and psychological or psychosocial intervention was not possible due to a lack of such studies.
Acupuncture treatment for postpartum depression
All three studies used different forms of acupuncture: standard acupuncture points (Chen et al, 2010), combination of standard acupuncture and threading scalp acupuncture (Dong and Gao, 2014) and acupuncture of Sun Si Miao's 13 ghost points (Yu et al, 2015). The acupuncture points used in two of the studies were similar standard points, chosen to strengthen the mother after labour and to enable smooth flow of qi. The additional threading scalp acupuncture was justified as assisting with managing the hormone imbalance in the postpartum period (Dong and Gao, 2014). Yu et al (2015) explained that Sun Si Miao's 13 ghost points are traditionally used for mental health conditions and the points were so named due to past beliefs that these conditions were caused by ghosts. The points are said to calm the mind and restore the balance of yin and yang to assist in postnatal depression.
Diagnosis of postnatal depression
As well as adopting a diagnosis according to the CCMD-3, the three studies used a cut-off of 17 for the HRSD, which indicates moderate-to-severe depression. However, while two of the studies mentioned the exclusion of ‘other mental or depressive disorders’ (Dong and Gao, 2014; Yu et al, 2015), none of the studies clearly stated whether participants suffering from depressive disorders were excluded before or during pregnancy. Furthermore, the onset of postnatal depression was not reported or mentioned in the inclusion/exclusion criteria. The DSM-IV states that the onset of postnatal depression will usually occur within 4 weeks of birth (American Psychiatric Association Task Force on DSM-IV, 2000), although postnatal depression studies have varied between 1 week and 1 year post-birth (Klainin and Arthur, 2009).
Postnatal depression is likely to be a culturally sensitive topic, which may have influenced the number of studies conducted. Halbreich and Karkun (2006) explain the prevalence of postnatal depression as it varies between different countries. Based on findings using the EPDS, a high prevalence was found in Italy, Korea and Taiwan (34–57%), while the USA and the UK was lower at 12.9–15.4%, but similar to China and Japan at 13.9–21.6%. The prevalence in Australia and New Zealand was even lower (9–10.1%), while in Singapore and Malaysia the prevalence ranged from 0.5–9%. The reason for such differences in prevalence may be due to multiple factors, including different attitudes and perception towards marriage, childbearing and depression, as well as varied availability of adequate healthcare services (Halbreich and Karkun, 2006). Stigma towards mental illness may also be a part of this picture, with more people of Asian or non-western backgrounds tending to refer to somatic symptoms rather than emotional problems (Klainin and Arthur, 2009). Certain cultures may also use traditional diagnostic terms to explain the condition, such as ‘wind or heat in the head’ or ‘anger disorder’ (Kim and Buist, 2005, Klainin and Arthur, 2009). Given that perception and expression of postnatal depression are deeply culturally embedded, the HRSD may not be valid as a measure of postnatal depression in Chinese populations. Furthermore, the ‘protective’ role of traditional practices after labour, such as receiving help from mother or mother-in-law and being confined at home for a period of time immediately after giving birth, is thought to be an influence on mood, but is as yet untested (Klainin and Arthur, 2009).
Implications for research
It is acknowledged that the small number of studies, small sample sizes, and presence of high risk of bias and high level of heterogeneity call for caution in interpreting these results. It is worth noting that acupuncture trials are inherently high for risk of bias due to the inability of blinding the clinician delivering the acupuncture treatment. It is also difficult to eliminate the placebo effect such as subjects' expectation and motivation for seeking and receiving complementary and alternative medicine. Recent efforts have aimed at clarifying the effect of acupuncture by improving study designs and/or developing a variety of sham acupuncture methods, including the invention of the Streitberger needle (Streitberger and Kleinhenz, 1998). The evidence remains limited on the topic; however, there are studies that indicate the presence of different biological effects between verum acupuncture and placebo acupuncture (Enck et al, 2010).
Larger, more rigorous studies with an equally strong focus on the safety of acupuncture need to be conducted to enable firmer conclusions. The scope of postnatal depression may also be broadened to include ante- and perinatal depression, considering that around 50% of women who experience postnatal depression show symptoms in the antenatal period (American Psychiatric Association, 2013). Future studies may also consider a more pragmatic approach that allows personalised acupuncture treatment, or integrated treatment of acupuncture and modern medication, in order to better reflect clinical practice. Furthermore, perinatal healthcare should be culturally responsive. Generalisability of results between Chinese and European samples need to be better explored and cultural factors better understood and taken into consideration. On another note, the HRSD may not be the most appropriate outcome measure tool for postnatal depression as it is conventionally used for major depressive disorders. The EPDS is a widely used, valid and reliable instrument, considered appropriate for use in postnatal depression, and it is surprising that none of the studies mentioned this. Future studies should consider comparing the validity and the contrasting findings of the HRSD and the EPDS.
Implications for the UK
This review was confined to studies conducted in China where acupuncture is a well-established treatment that many people receive regularly. In contrast, in the UK, acupuncture is not yet a widely practised therapy, although it is becoming more popular (particularly among women) and its demand is increasing for many health issues including depression (Hopton et al, 2012). Given the risk associated with pharmacological interventions, complementary and alternative therapies such as acupuncture are becoming important treatment options for perinatal depression (Deligiannidis and Freeman, 2014). In the UK and Australia, more GPs are in favour of acupuncture given in primary care and, in Australia in particular, many GP referrals are made for acupuncture (Wardle et al, 2013). In the UK, acupuncture is not commonly recommended by GPs, who play a role in postnatal care, including detection and assessment of postnatal depression (Ford et al, 2017). In the US, acupuncture is an increasingly accepted treatment and services are now provided in many conventional and academic medical centres (Eisenberg et al, 2016; Rhee et al, 2016; Borah et al, 2017). Given acupuncture's inherently safe nature as well as increasing popularity and demand in the UK, GPs may provide referrals or suggest acupuncture as an option for women with perinatal mental health issues, including postnatal depression.
Strengths and limitations
A strength of this review is its broad, deep and international scope of literature search, which included not only UK and Chinese databases, but also the Korean and Japanese databases. Despite the widespread search, only three studies matched the criteria for this study. Rigorous steps were adopted for extracting the data by using the CONSORT (Schulz et al, 2010) and the STRICTA (MacPherson et al, 2010; MacPherson et al, 2015) guidelines. The review is limited by the number of studies, small sample sizes and a presence of a high risk of bias. The variation in treatment protocols are a limitation of studies on acupuncture for depression (Wu et al, 2012). Another criticism is that because acupuncture follows the holistic approach of traditional Chinese medicine, treatment should therefore be personalised rather than standardised as was the case in these studies (Sniezek and Siddiqui, 2013).
Conclusion
Postnatal depression is a significant issue, and both practitioners and patients are searching for treatment strategies with the fewest side effects to the mother and baby. This review provides preliminary yet encouraging results showing that acupuncture may be well-tolerated and has the potential to play a role in the management of postnatal depression. It also updates the evidence of acupuncture to assist patients in making an informed decision. This review may act as an initial working platform to assist in moulding future rigorous studies and building stronger evidence.