
Hypertensive disorders of pregnancy (HDP) are classified as gestational hypertension, pre-existing or chronic hypertension and pre-eclampsia. HDP complicate 10% of pregnancies and the incidence of pre-eclampsia is 2-8% (Steegers et al, 2010). Pre-eclampsia is associated with adverse maternal and fetal outcomes, such as eclampsia, stroke, renal and hepatic dysfunction, intrauterine growth restriction, premature birth and stillbirth (Tranquilli et al, 2014; Townsend et al, 2015). The resources required for the monitoring of developing pre-eclampsia have significant cost implications (Stevens et al, 2017); however, the majority of women do not actually develop pre-eclampsia (Villar et al, 2003).
Traditionally, in the UK, women attend their scheduled antenatal visits as per National Institute of Health and Care Excellence (NICE) (2018) recommendations. If they show signs of HDP, or have risk factors for developing HDP, they will have extra scheduled antenatal visits to monitor for the development of pre-eclampsia. These extra antenatal visits could be with their GP, midwife or a health professional from a day assessment unit and the structure of care varies from hospital to hospital. Despite this increased surveillance of blood pressure, pre-eclampsia can manifest between antenatal visits, and so the diagnosis can be delayed until the next scheduled antenatal check (Waugh et al, 2001). Therefore, the traditional pathway may fail to capture women who may develop pre-eclampsia until it is at an advanced stage.
Some women may purchase their own blood pressure machine to monitor for the progression of pre-eclampsia with or without the support of a health professional (Lo et al, 2002). The literature claims that 30% of patients in the UK and up to 60% of patients worldwide monitor their own blood pressure without the guidance of a practitioner (Baral-Grant et al, 2012; McManus et al, 2014). These figures highlight the need for further research of home blood pressure monitoring (HBPM) in the pregnant population to meet the expectations of women and maintain safety standards in antenatal care.
St George's Hospital in London piloted an innovative care pathway for pregnant women at risk of developing pre-eclampsia with the implementation of HBPM and a smartphone app. The advantages of HBPM in the management of hypertension are well documented (Stergiou et al, 2004; Reims et al, 2005; Parati et al, 2010). Such advantages include:
Women were given a validated blood pressure monitor (Stergiou et al, 2007) on loan and were trained on how to use the machine accurately by a specialist hypertension midwife. There was also a training video on the app, demonstrating how to measure blood pressure accurately, to which women could refer at a later date. Women were instructed to monitor their blood pressure approximately once per day, depending on the severity of their hypertension. Users were required to insert their blood pressure results into a downloadable mobile app and answer trigger questions for symptoms of pre-eclampsia, such as ‘do you have headache?’. If the user inserted any abnormal blood pressure ranges (≥150 mmHg systolic or ≥100 mmHg diastolic) or answered ‘yes’ to the trigger questions (headaches, visual disturbances or upper abdominal pain), a red message was flagged to the user's mobile screen, advising the user that their results were out of normal range and to contact their midwife or hospital. These women had a reduced appointment schedule compared to the traditional schedule for someone at risk of pre-eclampsia (NICE, 2018) and were followed up approximately every 2 weeks in the midwife-led hypertension clinic. This care pathway provided continuity of care to women—unlike the traditional pathway, where it is common for women to see a different practitioner at each visit.
The main aim of this research was to explore women's experiences of using the HBPM service. The secondary objectives were to assess patient satisfaction, and their acceptability of HBPM and a reduced hospital schedule.
Methods
This qualitative study used a grounded theory approach (Strauss and Corbin, 1990). Grounded theory is indicated when there is little known about a topic and the aim of the study is a generated theory with explanatory power (Birks and Mills, 2011). This approach was indicated as there was a significant gap in the literature related to women's experiences of HBPM in pregnancy.
As a midwife, the researcher (ES) was interested in listening to women's stories to influence future practice. This allows the researcher to interpret women's experiences and provide information that can enhance patient satisfaction and quality of care. The researcher is therefore aligned to the interpretivist paradigm, which means seeing reality as an interpretation of human understanding (Fossey et al, 2002). The grounded theory approach (Strauss and Corbin, 1990) is influenced by symbolic interactionism, which means that it is focused on interpreting human actions or experiences (Blumer, 1969).
Grounded theory goes beyond basic description and the end product is a rich interpretation of the data following a systematic grounded theory method (Denscombe, 2014). The aim of grounded theory is to produce a substantive or formal theory (Glaser, 2007).
Setting
Women were recruited from an antenatal hypertension clinic in a London teaching hospital. In addition to the hypertension clinic, there was a day assessment unit, to which women could be referred by their community midwife or GP for hypertension.
Participants
Women who had a HDP were recruited through purposive sampling. The sample size is unknown to the researcher at the beginning of grounded theory research, as the numbers required are dependent on data or theoretical saturation, when there are no new themes emerging (Charmaz, 2006). The researcher sent postal invitations with a patient information leaflet to 48 women who met the inclusion criteria. There were 17 responses received, with 11 women agreeing to participate and 6 declining to participate. A total of 8 women were interviewed as theoretical saturation was achieved with no new data emerging. The remaining three women were contacted by the researcher explaining that they were no longer needed and thanking them for their time and consideration. Six interviews took place in the participants' homes and two interviews took place at the maternity hospital as per the participants' request.
Data collection
Ethical approval was granted by the East of Scotland research ethics service. Approval was sought from the NHS hospital management and risk team as the study included NHS patients.
The main method of data collection was via semi-structured interviews using mainly open ended questions to allow maximum description of experiences and explanation from the participants. Semi-structured interviews are recommended in grounded theory (De Chesnay, 2014; Stern and Porr, 2011), as structured questions would fail to capture the natural emergence of data and unstructured questions could be confusing for a novice researcher who may not have the experience to direct the interview appropriately to gather rich data. The researcher transcribed all interviews verbatim.
Data analysis
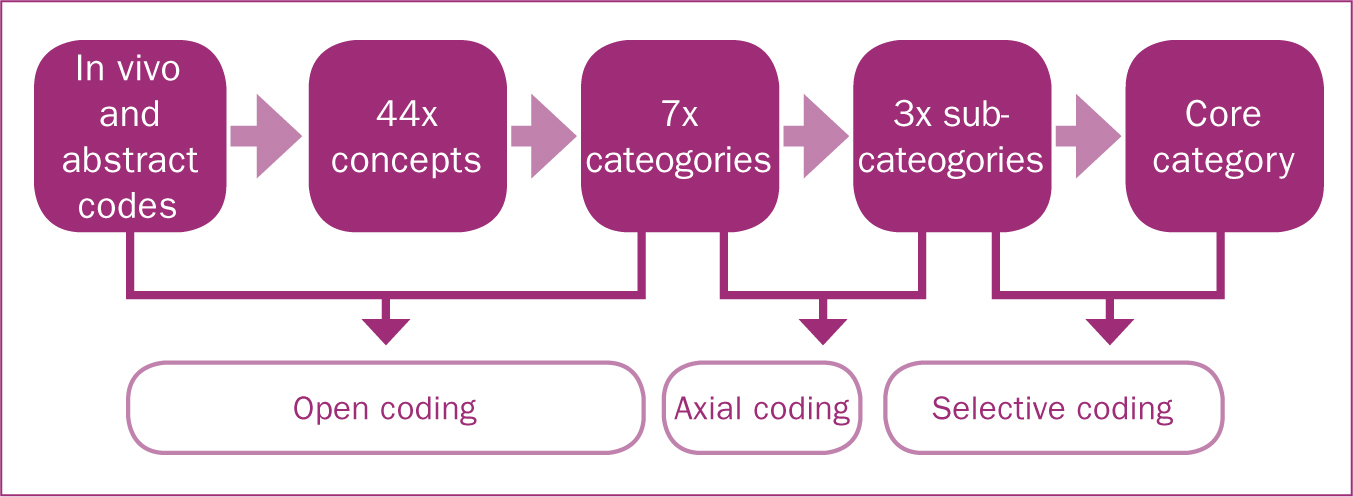
The first interview was analysed for concepts or emerging ideas and was compared with the other interviews by using the constant comparison method. The constant comparison method, whereby data is continuously analysed and compared to previous data analysis for similarities or differences throughout the data collection and analysis process, is unique to grounded theory research (Strauss and Corbin, 1990). Memos were created after each interview to identify emerging concepts and were used as data. All data was analysed by a process of coding by Strauss and Corbin (1990) including open, axial and selective coding (Figure 1). At the end of open coding, where the data is analysed line by line, the researcher was left with seven categories that needed to be analysed further by axial coding (Flick, 2009). This is where the researcher looks at the codes and categories from a different perspective or ‘turns the codes on their axes’ (Olshansky, 2015: 22), looking for different meanings. In this study, the researcher went back to the raw data and compared the codes with the seven categories using coloured ink pens to match up the data. Selective coding is the process of refining the theory even further by selecting a core category (Strauss and Corbin, 1990). The core category was selected by identifying the theme that most represented what the participants were saying in their interviews. The subcategories were chosen to demonstrate key topics or themes that best answered the research question. The researcher's academic supervisor (LK) also analysed the data independently and discovered similar findings.
Findings
A total of 8 women were interviewed. Participants completed at least 8 weeks of HBPM using the innovative care pathway. All participants were aged between 30 and 41 years old (Table 1).
| Participant | Age | Ethnicity | Parity | Diagnosis |
|---|---|---|---|---|
| 1 | 37 | Caucasian | 0 | Chronic hypertension |
| 2 | 38 | Caucasian | 0 | White coat hypertension |
| 3 | 35 | Asian | 1 | Previous severe pre-eclampsia |
| 4 | 34 | Caucasian | 0 | Gestational hypertension |
| 5 | 30 | Black | 1 | Chronic hypertension |
| 6 | 41 | Caucasian | 2 | White coat hypertension |
| 7 | 32 | Caucasian | 0 | Gestational hypertension |
| 8 | 36 | Caucasian | 1 | Previous HELLP syndrome |
HELLP: Haemolysis, Elevated Liver enzyme, Low Platelet
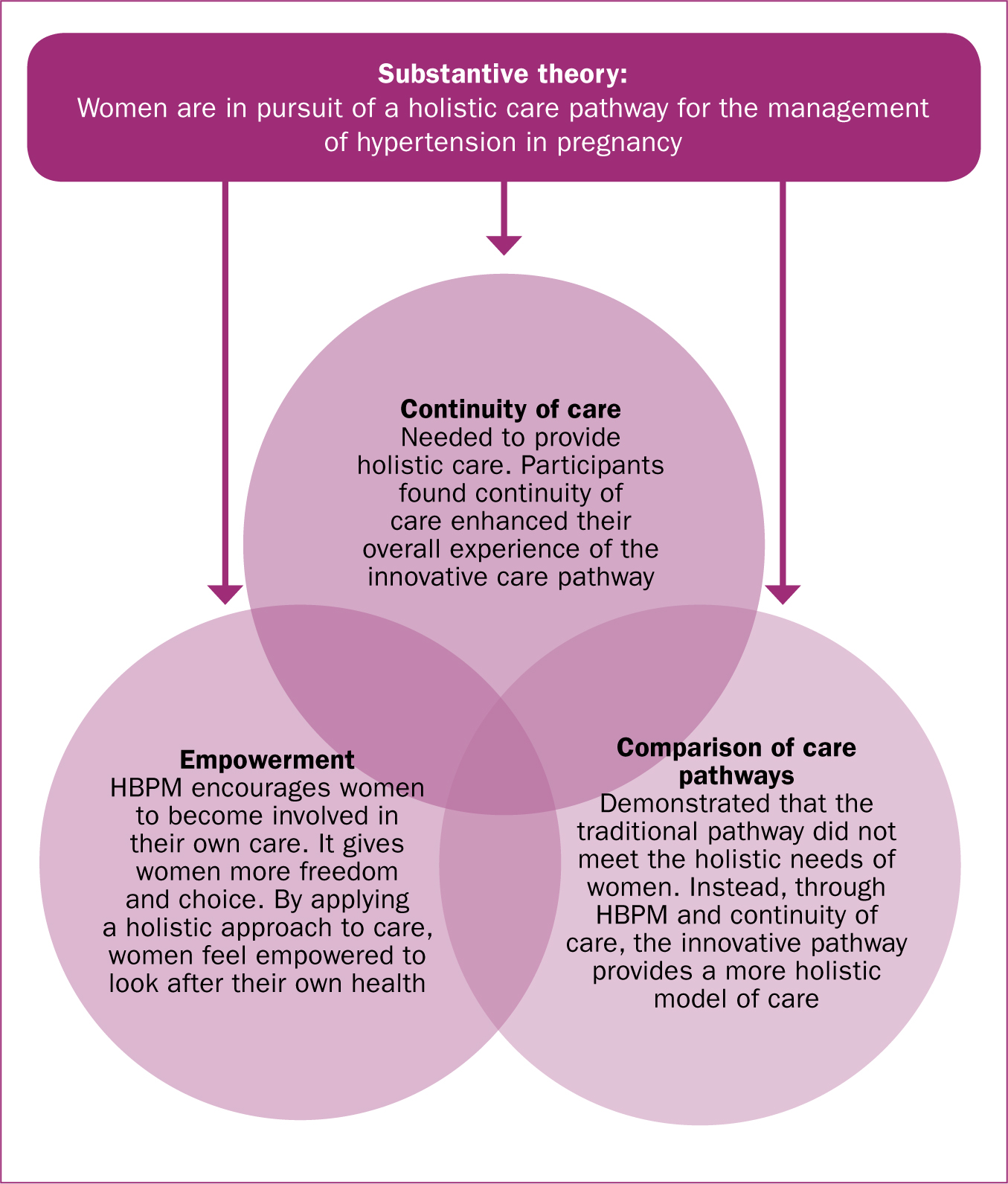
The core category was identified as ‘holistic care’ with ‘empowerment,’ ‘comparison of care pathways’ and ‘continuity of care’ emerging as the subcategories. Holistic care was identified as having the most explanatory power for the subcategories, while the subcategories reflected what the women focused on when sharing their experiences of an innovative care pathway. The substantive theory was interpreted by the researcher as ‘women are in pursuit of a holistic care package for the management of hypertension in pregnancy’ (Figure 2). This emergent theory formed the foundation of the core category, ‘holistic care’.
Core category: holistic care
The researcher interpreted from the participants' interviews that women were in pursuit of a holistic care pathway for the management of their hypertension. Although participants described mainly positive experiences with the innovative care pathway, they also highlighted what could be improved. For example, some participants described inadequate postnatal care and said that they would have liked to continue seeing the same midwife or team during the postnatal period:
‘The prenatal care was much better than the postnatal care for lots of different reasons … I do think there is a cut off … I think it would be nice to close the loop.’ (Participant 7)
‘They put all that money into seeing me during pregnancy to make sure I got to that point OK and I'm very happy, but we had a really tricky start … I would have liked to have gone back and seen the same team.’ (Participant 1)
It appeared that patient satisfaction could have been improved if these participants had received continuity of care in the postnatal period. The researcher interpreted that a holistic care pathway could address this concern.
One participant explained how the innovative pathway was tailored to her individual needs:
‘I felt like I was looked after holistically and I was seen as an individual … especially when I came in, I was always given a chance to allow my blood pressure to calm down and recheck it or even check it at home as well.’ (Participant 7)
Creating a care plan that reflects what women want will not only increase patient satisfaction, but will also empower women to become actively involved in their own care.
Empowerment
It was clear from the data that women wanted to be involved in their own care and wanted to see and know what their blood pressure measurement was. The HBPM pathway demonstrated its ability to reassure women about their blood pressure and alleviate their anxieties.
‘I felt happier knowing that I checked it everyday … For me actually knowing what [my blood pressure] is, was such peace of mind … I could rationalise it and think, ‘It's alright, there isn't actually a problem here’ … so yeah, it helped me hugely.’ (Participant 2)
Women felt that HBPM gave them some control over their care, reflecting their willingness to be involved in their hypertension management:
‘It didn't make me feel nervous; if anything it made me feel in control of my own health and knowing what was low and high and what to do, and that could be any day or time that you like.’ (Participant 7)
All participants referred to self-awareness of their hypertension or to knowledge they had acquired from HBPM. The researcher interpreted that this knowledge empowered them to become involved in their own care. This empowerment explained how and why women were in a position to take an active role in managing their hypertension. It is important for health professionals to acknowledge these abilities and encourage women to feel empowered, in order to enhance patient experience. In doing so, women will feel like their holistic needs are being met, which will then increase patient satisfaction.
Comparison of care pathways: HBPM vs the traditional model
The researcher did not intend to compare the innovative care pathway with the traditional care pathway for the management of hypertension; however, this subcategory emerged purely from the raw data itself. Although the participants completed the innovative care pathway, some women recalled their previous experiences with other pregnancies when they were under the traditional pathway. Likewise, the participants in their first pregnancy recalled experiences in early pregnancy before they were referred to the innovative care pathway, where they experienced the traditional model of care.
Participants described their experiences with the traditional model and compared their experiences with the innovative model:
‘There was no place for them to take us, so I remember being sat in this corridor while they took my BP [blood pressure] … and telling them, ‘I don't think having [my blood pressure] read in this busy corridor full of lots of people, some of them very stressed … I don't think this is the most appropriate place to be taking my blood pressure and won't give a clear reading anyway.’’ (Participant 2)
Soon after this experience, the patient was referred to the innovative care pathway, under which she was allowed to monitor her blood pressure at home and have follow up in the specialist hypertension clinic with continuity of carer. The same participant reported on the HBPM pathway:
‘I was so so grateful for the [hypertension] clinic existing and having that option [HBPM] … I mean, this isn't over the top, but I think it really made a huge difference to my whole experience of pregnancy and being pregnant.’ (Participant 2)
It was evident how the switch from traditional care to a holistic approach enhanced this participant's experience.
Similarly, another participant was advised to have weekly blood pressure checks with her GP between routine hospital appointments before she was started on the innovative HBPM pathway. The GP was unable to accommodate the patient and advised a walk-in centre.
‘[HBPM] did make a difference because prior to the HBPM … my GP sent me for a walk-in once and I had to wait like 2 or 3 hours and that was just stressful because I was pregnant and there was coughing and sick people everywhere and it was just horrible … it was stressful before I got the app … it absolutely made a difference.’ (Participant 4)
The accounts of women's experiences before HBPM demonstrate fragmented care with no-one taking responsibility or considering the woman's needs.
Continuity of care
The topic ‘continuity of care’ had a strong presence in the data. The innovative care pathway meant that women had continuity of care with one midwife during their pregnancy. However, once they gave birth, their postnatal care was under the traditional shared care model between community midwives and their GP. It appeared that continuity of care was what women valued the most from being under the innovative care pathway:
‘What I found fantastic, which was really key to me, was the continuity of care with seeing the same two midwives in my case was excellent and I felt like I was in good hands … if anything were to go wrong at least there will be qualified people to help me and that just made all the difference.’ (Participant 8)
‘When you're pregnant, it's a weird vulnerable state, there's a massive change in your life and in your body … and just being able to see the same person, you build up a kind of relationship and they know your situation and they know you, and they don't have to read over your notes … it was really nice.’ (Participant 2)
The literature also shows that continuity of care is something that women want in general, not just in cases of hypertension (Homer et al, 2002).
Some participants felt more strongly than others about continuity of care for hypertension and for postnatal care:
‘When you're out of hospital there didn't seem to be a clear, blood pressure postnatal, sort of, system … you're high risk and have all these complicated stuff going on, my team know what's going on and what's been happening and then it feels like you can't really access that stuff again so that continuity seems a bit pointless.’ (Participant 1)
This participant was evidently frustrated with the postnatal approach to managing her hypertension. A holistic approach would have addressed this woman's concerns by providing access to continuity of care into the postnatal period.
Discussion
Interpretation of the raw data showed that women wanted a holistic approach to the management of their hypertension. Some participants reported that their postnatal care was inadequate and they suggested how having continuity of care in the postnatal period could address this. In contrast, other participants reported they did in fact feel like they were looked after holistically. HBPM was identified as a factor in yielding holistic care as it allowed white coat hypertension to be identified and managed appropriately, helping women to avoid long waiting times in a day assessment unit. HBPM also provided reassurance to women with hypertension by showing them that their blood pressure was within target or that they were advised to contact their hospital. HBPM addressed the uncertainty and anxiety that women might have between scheduled antenatal appointments under the traditional pathway by providing more regular blood pressure readings.
When interpreting women's experiences of the service, all data linked back to holistic care. There were certain aspects of the service women liked, such as care plans that were specific to their hypertension diagnosis, as well as other aspects that women did not like, such as the lack of continuity of care in the postnatal period. Healthcare providers are therefore encouraged to listen to service users and provide a holistic care package that addresses the needs of women for the future management of hypertension in pregnancy.
Themes identified
Empowerment
The research showed that the innovative care pathway empowered women to become involved in their own care. Women reported feeling confident in managing their own health at home and explained that this confidence was linked to self-awareness or knowing themselves best. Participants demonstrated a willingness to be involved in their care and were content to do so. This fits with the findings of the study by Fletcher et al (2016), which showed that patients felt empowered to manage their blood pressure and were less likely to attend their GP for management of their hypertension. In this study, participants were also content to have fewer hospital follow-up appointments. However, Fletcher et al (2016) reported that both patients and clinicians felt uncomfortable in interpreting blood pressure results. This was not suggested in this study's findings, possibly due to a smaller sample, continuity of care and a holistic approach. Continuity of care means fewer clinicians caring for patients, fewer opinions and fewer different interpretation of results. The holistic approach in this study ensured that women were informed of their target blood pressure and warned if their blood pressure did not meet this target. Furthermore, women's understanding of how to check their blood pressure and what to do on discovering a high reading was assessed before they were allowed to participate in the innovative pathway.
Comparison of pathways
Participants shared their experiences of both the innovative and traditional care pathways, and it was evident that all participants were strongly in favour of the innovative care pathway. Women associated the traditional pathway with long waiting times, multiple carers and sub-optimal management of hypertension, and so were keen to stay out of hospital and manage their hypertension as an outpatient. This is similar to findings in the literature where the majority of participants preferred outpatient management of their hypertension to frequent hospital follow-up appointments. Ross-McGill et al (2000) found that most women accepted HBPM and preferred a reduced appointment schedule with HBPM in future pregnancies. In addition, studies investigating acceptability of HBPM in the non-pregnant population also found that the majority of participants preferred reduced schedules and HBPM (Ganapathy et al, 2016; Lan et al, 2017). Although it is speculative, it is worth noting that respondents had a choice to participate and thus, acceptability of HBPM in these studies does not reflect the opinion of those who declined to take part.
However, with advances in technology and the majority of women of childbearing age owning a smartphone (BabyCentre UK, 2012), it is no surprise that women are accepting of this innovative service and technology. In an era that is powerfully influenced by technology, perhaps now is the time to take advantage of this opportunity and start transforming traditional pathways no longer fit for purpose to innovative pathways that meet the holistic needs of women.
Continuity of care
Continuity of care is very important to women and it appears to be the primary cause of patient satisfaction with the service. Although this not an expected finding in this study, it has been well documented in the literature (Homer et al, 2002; Roberts et al, 2017). Women found that continuity of care in the antenatal period was the key to their overall satisfaction and experience of the innovative model; however, some women also felt that they lacked continuity of care in the postnatal period, highlighting women's pursuit of a holistic care pathway. This is in line with the study by Roberts et al (2017), which found that continuity of care positively influenced their experience. They recommended that women with high-risk conditions of pregnancy, such as hypertension, should be cared for through a multi-disciplinary continuity of care model. This is similar to the model of care provided to women in this study, which also demonstrates that such a model of care can be achieved.
Relevance to practice
This study has identified inconsistencies with the traditional management of hypertension in pregnancy. It is the role of the midwife to provide holistic care for the women in their care (Nursing and Midwifery Council (NMC), 2018). Midwives cannot fulfil this task under the traditional care model, as it is not reflective of holistic care. Women are in pursuit of a holistic care pathway that will meet their physical, emotional, social, economic and spiritual needs, and this study provides evidence to transform the traditional model to a holistic one. The results from this study could be used to provide better care for women with hypertension by implementing continuity of care into the postnatal period. Furthermore, these findings will support the proposal to implement HBPM into local hospital guidelines for the management of hypertension in pregnancy.
Limitations
This was a small, single centre study. The approach to the management of hypertension in pregnancy will be different in each hospital and therefore the traditional model in this study may not be representative of other hospitals' management of hypertension. This study was not randomised and therefore women had a choice to participate in the innovative care model, meaning that these findings are from women who may have had a preference for HBPM and reduced hospital appointments. Furthermore, as a novice researcher who did not have any experience in interview technique, it is plausible that the researcher did not capture as much rich data as an experienced grounded theorist would.
Recommendations for further research
Only 1 woman developed mild pre-eclampsia in this study, which is in line with a small study sample and the fact that the majority of women do not develop pre-eclampsia. This study did not capture the effect that identifying signs of pre-eclampsia at home had for pregnancy outcomes. A large clinical trial is recommended to assess the association between HBPM and mortality and morbidity in the high-risk pregnant population. A larger qualitative study could also capture the experiences of women with sub-optimal outcomes (who were purposely excluded in this study), as these women may bring a different perspective to HBPM and the innovative care pathway.
Conclusion
Women in this study reported that their experience of an innovative care pathway using a smartphone app was positive overall. Women accepted HBPM and welcomed a reduced hospital schedule. There was increased patient satisfaction associated with the innovative care pathway in comparison to the traditional pathway, mainly due to continuity of care and reduced hospital appointments. The traditional care pathway is associated with long waiting times, busy and stressful environments and multiple carers, leading to multiple different opinions on the management of hypertension in pregnancy, which leaves women confused, anxious and stressed. The innovative care model is associated with continuity of care, reduced hospital appointments and women becoming actively involved in their care; however, continuity of care is lacking in the postnatal period, leaving women unsure about the management of hypertension.
Women are in pursuit of a holistic care pathway to manage their hypertension. Participants highlighted what worked and what did not, and the issues associated with the traditional pathway were made clear. The traditional pathway is no longer fit for purpose as it does not meet the holistic needs of women. The innovative model is not perfect and it needs improvement, but it is a step in the right direction towards holistic care. The findings have contributed to knowledge and evidence for future developments in the management of hypertension in pregnancy. This evidence has implications for future practice that can be addressed at both a local and national level. This study has demonstrated that the provision of a holistic care model for the management of hypertension in pregnancy is realistic and achievable.