References
Improving the culture of care


Abstract
Kate Nash, Senior Lecturer and Professional Midwifery Advocate, provides an overview of the advocating for education and quality improvement (A-EQUIP) model and role of the Professional Midwifery Advocate
Consideration is given to how the Professional Midwifery Advocate (PMA) role can serve as a catalyst for change and help drive improvement within maternity services as it promotes the development of a positive learning culture and compassionate care. The significance of advocating for education and quality improvement (A-EQUIP) and potential that the PMA role has to contribute to the transformation of maternity services is emphasised.
The A-EQUIP model incorporates the four functions presented in Figure 1 which provide the framework for the PMA role. These are normative, formative, restorative and personal action for quality improvement. An overview of these four functions is provided in Table 1.
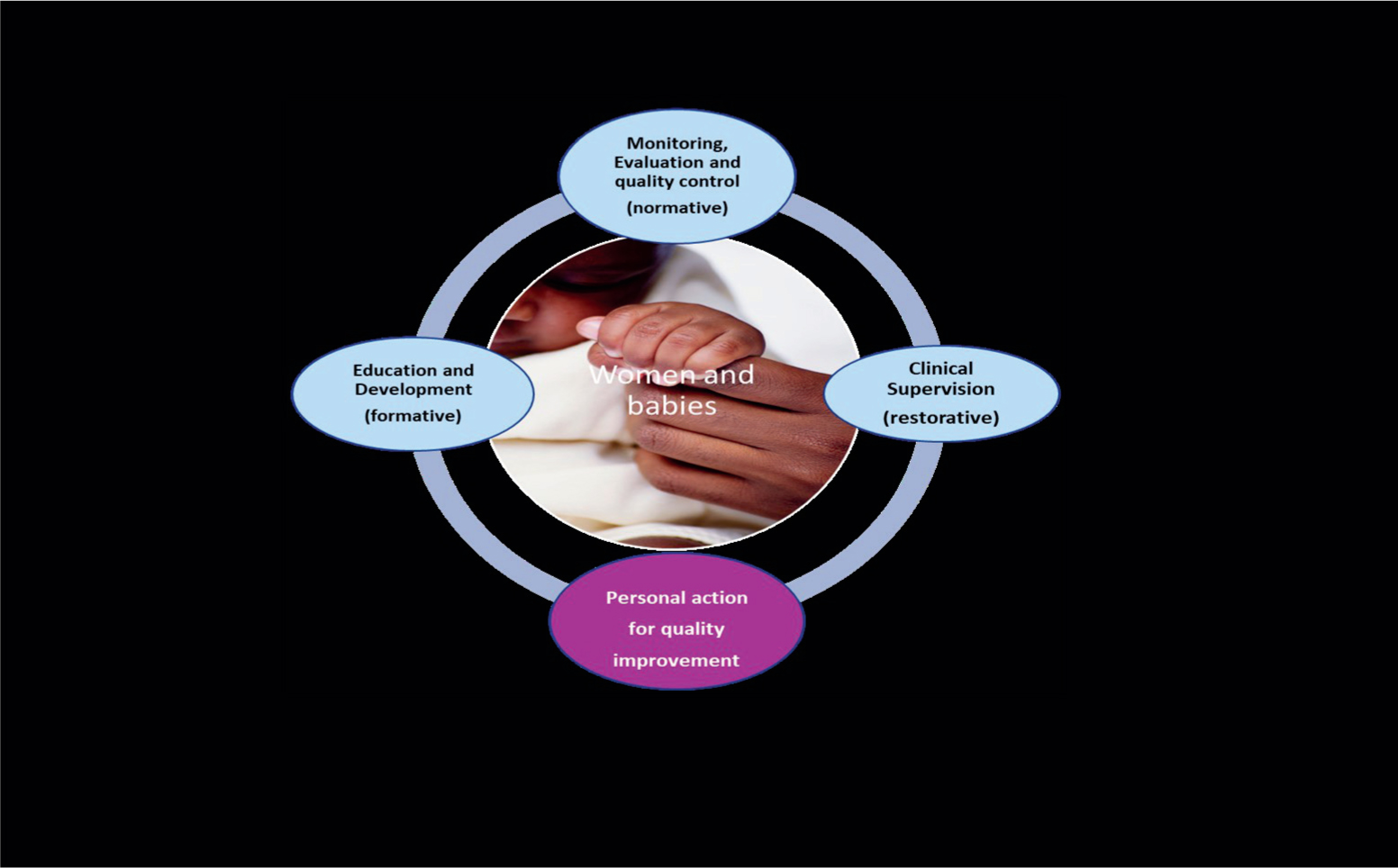 Figure 1. A-EQUIP model
Figure 1. A-EQUIP model
Based on one of the most commonly used clinical supervision frameworks (Proctor, 1986) with the addition of the fourth function, ‘personal action for quality improvement,’ (NHS England, 2017) A-EQUIP should be used as a tool for optimising personal and professional accountability, facilitating professional development, supporting staff wellbeing, and contributing to a learning and compassionate care culture.
Register now to continue reading
Thank you for visiting British Journal of Midwifery and reading some of our peer-reviewed resources for midwives. To read more, please register today. You’ll enjoy the following great benefits:
What's included
-
Limited access to our clinical or professional articles
-
New content and clinical newsletter updates each month