
The incidence of diabetes mellitus is increasing, alongside the increased prevalence of obesity, sedentary lifestyle, older age at conception and younger age at onset of type 2 diabetes, meaning that more women are pregnant and have diabetes (McCance et al, 2011; National Institutes of Health, 2013; Guariguata et al, 2014).
As midwives are often the first point of contact for women during pregnancy, the following article aims to provide a concise, practical review, from the first visit to the postnatal period. The article is aimed at both community and hospital-based midwives and gives an overview of care with relevant supporting evidence.
Wherever possible, the authors recommend referring to local guidelines for specifics of care. Until 2009, glycated haemoglobin (HbA1c) was solely reported in Diabetes Control and Complications Trial units (%). To standardise reporting across the world, the International Federation of Clinical Chemistry units (which report HbA1c as mmol/mol) were introduced and adopted in the UK in 2009. HbA1c is reported in both formats throughout this article. Women who have type 1 or type 2 diabetes before pregnancy are referred to as ‘pre-existing diabetes’, but distinguished where necessary.
Importance of glycaemic control in pregnancy
Women without previous diabetes
Two landmark studies, the Hyperglycaemia and Adverse Pregnancy Outcome (HAPO) trial (HAPO Study Cooperative Research Group et al, 2008) and the Australian Carbohydrate Intolerance Study in Pregnant Women (ACHOIS) trial (Crowther et al, 2005) have shown adverse outcomes in women and babies, associated with escalating degrees of hyperglycaemia.
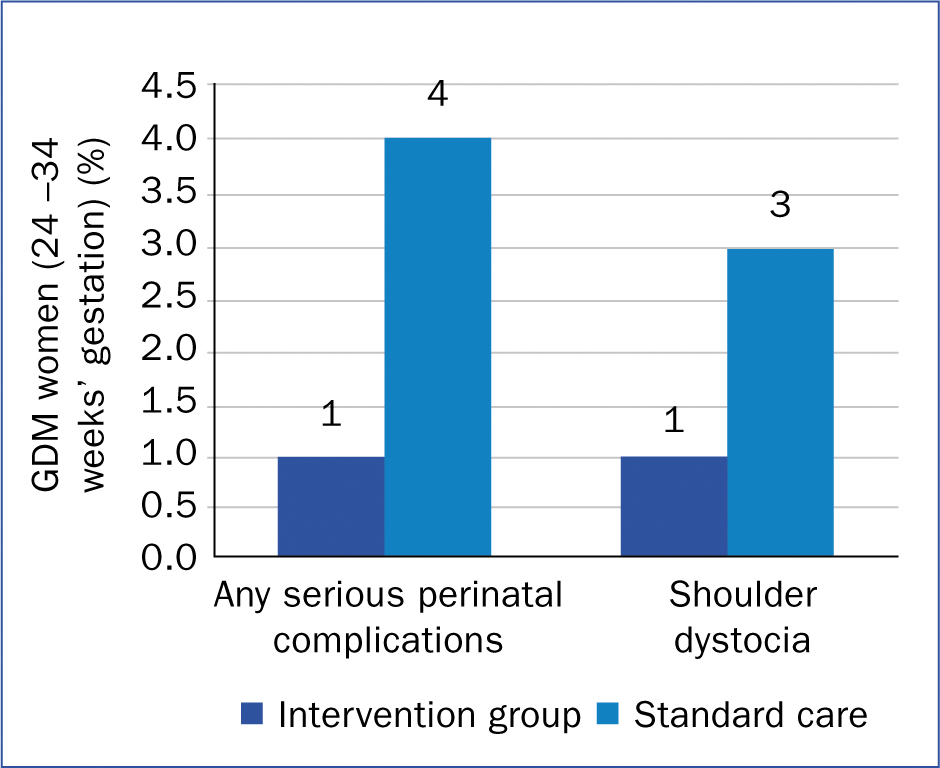
The ACHOIS study (Crowther et al, 2005) showed that pregnant women with what was considered at the time as ‘mild’ gestational diabetes (2-hour value after 75 g oral glucose tolerance test (OGTT) between 7.7 and 11.1 mmol/L) had improved outcomes when treated intensively with diet or insulin (Figure 1) (IDF diabetes School, 2019).
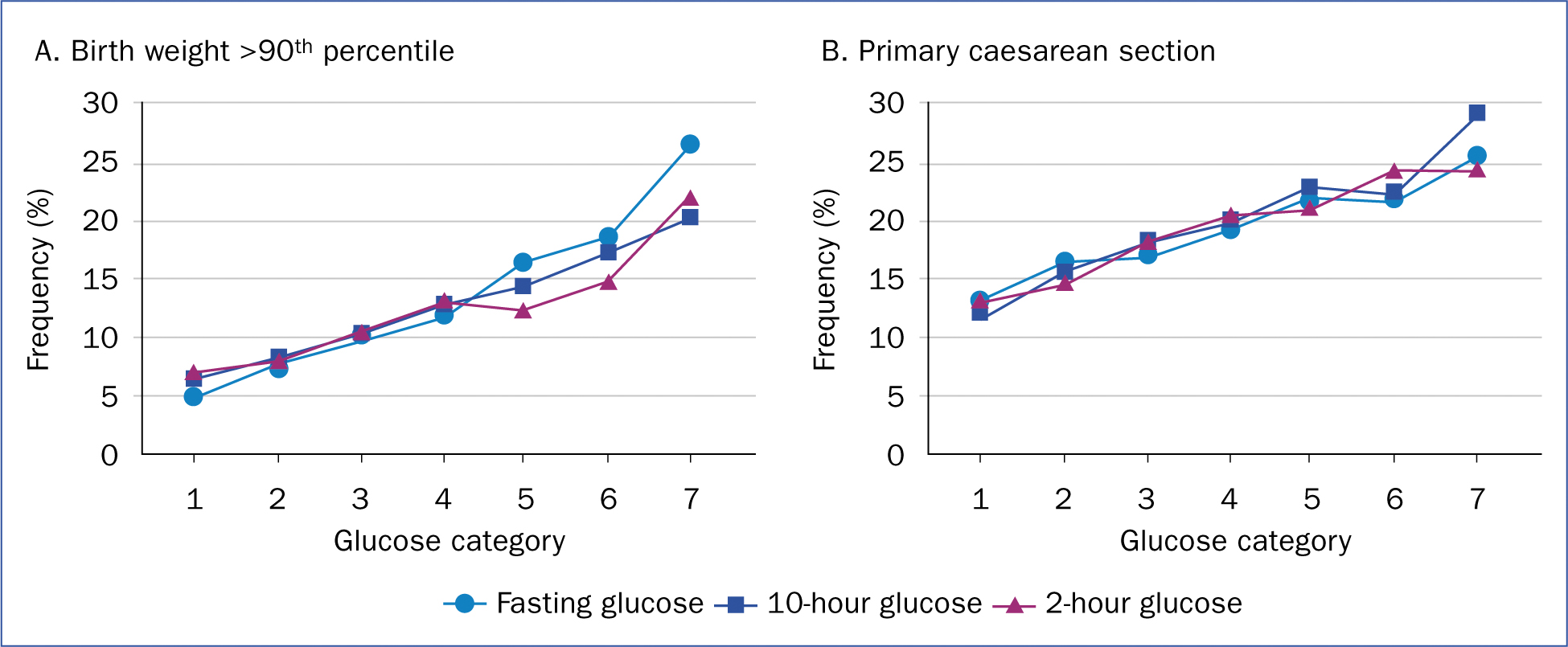
The HAPO (HAPO Study Cooperative Research Group et al, 2008) study also included women without diabetes, tested with a 75 g OGTT between 24 and 32 weeks of pregnancy. Outcomes measured included the impact on fetal birth weight, neonatal hypoglycaemia, rates of caesarean section and fetal insulin levels. The study showed that adverse pregnancy outcomes increased in parallel with increasing glucose values, even in ranges that had historically been considered normal (Figure 2). It was determined that the risks to pregnancy were most evident with fasting glucose levels of 5.1 mmol/L, a 1-hour glucose value of 10 mmol/L and a 2-hour value of 8.5 mmol/L. The results of these studies paved the way for the ‘tighter’ blood glucose targets in pregnancy that are in use today.
The HAPO follow-up study (Scholtens et al, 2019) showed that exposure to increased glucose levels in utero also had long-term consequences for babies as they themselves grew to develop glucose intolerance and insulin resistance.
Women with previous gestational diabetes
Women with a history of gestational diabetes mellitus (GDM) are at an increased risk of developing GDM in future pregnancies, often at an earlier stage. These women should therefore be screened for diabetes as soon as practicable early in the pregnancy.
Once GDM is diagnosed, there is the associated risk of hypertensive disorders in pregnancy, such as gestational hypertension, pre-eclampsia, chronic hypertension and eclampsia (Caughey, 2018). The reason for this association is not clear, although both conditions are associated with insulin resistance, maternal fat deposition patterns and overweight/obesity.
Gestational diabetes mellitus
Maternal obesity and/or hyperglycaemia that occurs in GDM can lead to fetal macrosomia (Ehrenberg, 2004). This is thought to arise partly from the trophic effect of high insulin levels produced by the fetus in response to hyperglycaemia, and explains the importance of controlling postprandial glucose in pregnancy.
During childbirth, fetal macrosomia increases the risk of shoulder dystocia, Erb's palsy, brachial plexus trauma and clavicle fracture. The pattern of fat deposition in the infant (the inter-scapular and abdominal areas) may contribute to this (Kc et al, 2015)
Fetal macrosomia carries other risks to the baby, including hypoglycaemia and jaundice (Kc et al, 2015), as well as risks to the mother, such as increased rate of caesarean section, postpartum haemorrhage and perineal tears (Kc et al, 2015).
Pre-existing diabetes
Hyperglycaemia in the first trimester can damage the embryo, often before a woman knows that she is pregnant. This could then increase the risk of spontaneous abortion, fetal anomalies, pre-eclampsia and fetal death (Evers et al, 2004; Confidential Enquiry into Maternal and Child Health, 2005). This explains the importance of pre-conception care. During the second and third trimesters, hyperglycaemia can also put the infant at risk of fetal macrosomia, with the same complications as outlined above.
Preconception care
All women with pre-existing diabetes should ideally receive preconception care. Box 1 explains what one needs to go through in pre-conception clinic.
First trimester
Screening
If a woman has a previous history of GDM, National Institute of Health and Care Excellence (NICE) guidelines recommend that screening should take place at the booking appointment with self-monitoring of blood glucose or 75g OGTT (NICE, 2015a; American Diabetes Association, 2018).
Alternatively, if glycosuria of ≥1+ on two or more occasions is present, or ≥2+ just once, then further testing with a diagnostic test is needed to determine the presence of GDM (NICE, 2015a).
The method used for the diagnostic test varies from the 75 g OGTT to a random HbA1c and random blood glucose test, depending on local guidelines. NICE (2015a) criteria define GDM as fasting glucose ≥5.6 mmol/L and 2-hour glucose, after 75 g OGTT, ≥7.8 mmol/L. Be aware that a first trimester HbA1c value ≥48 mmol/mol (6.5%) or random plasma glucose of ≥11.1 mmol/L not only diagnoses GDM, but is also highly suggestive for pre-existing type 2 diabetes (American Diabetes Association, 2018)
If a first-trimester diagnostic test is not in the range for GDM, tests should be repeated with 75 g OGTT or self-monitoring of blood glucose (Metzger et al, 2010; NICE, 2015a) at 24-28 weeks' gestation (Metzger et al, 2010; American Diabetes Association, 2018).
Women without previous GDM, but who have risk factors (NICE, 2015a) to develop GDM are screened at 24-28 weeks' with 75 g OGTT or self-monitoring of blood glucose (Metzger et al, 2010; NICE, 2015a; American Diabetes Association, 2018). These risk factors are any of the following:
Glycaemic targets
Glycaemic targets are no different between GDM and pre-existing diabetes. NICE advises aiming for fasting glucose <5.4 mmol/L. One hour after meals, the target is <7.9 mmol/L. If measured 2 hours after a meal, then aim for <6.5 mmol/L (NICE, 2015a). Always refer to local guidelines for glycaemic targets. The best way to assess glucose levels is through self-monitoring of blood glucose. HbA1c is useful and gives an overview but is not as responsive to rapid changes in insulin doses. The target HbA1c in pregnancy is 42–48 mmol/mol (6–6.5%) but may be relaxed to 53 mmol/mol (<7%), if necessary to prevent hypoglycaemia.
A note on diabetes medications in pregnancy
Metformin is widely used in GDM. Rowan et al (2008), randomised women with GDM at 20–33 weeks' gestation to receive either metformin (plus insulin if required) or insulin alone. Just under half of those given metformin needed to have insulin as well. Overall, outcomes were no different between groups, suggesting that metformin is safe.
Metformin is offered to women with GDM if blood glucose targets are not met after changes have been made to diet and exercise. However, immediate treatment with insulin, with or without metformin, should be offered to women with fasting plasma glucose level of 7.0 mmol/L or above at diagnosis, or to women with fasting plasma glucose is between 6.0–6.9 mmol/L with complications such as macrosomia or polyhydramnios. This is in order to optimise glycaemic control in order to achieve maximum benefit in pregnancy (NICE, 2015a).
There are long-term safety data on the use of human insulin in pregnancy and is the preferred long-acting insulin according to NICE (2015a) guidelines. Analogue insulins can be continued if they were used before pregnancy (NICE, 2015a).
NICE (2015a) approved the use of glibenclamide for GDM when neither metformin nor insulin could be tolerated or were acceptable to the woman; however, caution is advised, as long-term safety data are lacking. Increased levels of glibenclamide are found in cord blood and its use may result in fetal macrosomia and neonatal hypoglycaemia (Balsells et al, 2015).
Booking appointment
Women without diabetes
Women who are not known to have diabetes should receive routine antenatal care. Box 2 lists points to follow during their booking visit.
Women who are diagnosed with GDM through these tests should be seen by members of the joint diabetes and antenatal care team within 1 week of diagnosis. These women should also be offered folic acid 5 mg once daily and vitamin D supplements.
Women with pre-existing diabetes
Pregnant women should be referred to a joint antenatal-diabetes clinic at the earliest opportunity (NICE, 2015a). An ultrasound scan to confirm viability of pregnancy is performed at 7-9 weeks' gestation. The two main aims at booking are ensuring that medications are optimised and that screening processes are in place for suspected complications, such as nephropathy and retinopathy.
The mother should be taking folic acid supplements at 5 mg daily and vitamin D supplements (10 micrograms daily) (NICE, 2015a). Unless specifically stated, women should not be on angiotensin converting enzyme (ACE) inhibitors, angiotensin-II receptor blockers (ARBs) or statins (NICE, 2015a). Discuss starting aspirin at 10–12 weeks' to reduce the risk of pre-eclampsia (Metzger et al, 2010)—this will then be continued throughout pregnancy. All oral hypoglycaemic agents, other than metformin, should be stopped (NICE, 2015a). It is safe to continue any form of insulin if women were taking it before pregnancy (NICE, 2015a), but it is vital that women are aware of how to recognise and self-treat hypoglycaemia. Women with type 1 diabetes should be issued with a ketone meter, with advice to check for ketones if they become unwell or hyperglycaemic (blood glucose ≥13 mmol/L) (Diabetes in Pregnancy Advisory Group, 2010; NICE, 2015a).
The clinical records should be checked for diabetes complications (such as retinopathy, nephropathy, neuropathy and cardiovascular disease) (NICE, 2015a) and blood pressure measured (targets shown in Box 1). Arrange diabetes eye screening via local care pathway as soon as possible, unless this has occurred in the previous 3 months (NICE, 2015a). Similarly, unless urine albumin creatinine ratio (ACR) and serum creatinine have been measured in the preceding 3 months, send off a sample to the laboratory as soon as possible (NICE, 2015a). If urine ACR >30 g/L or creatinine >120 µmol/L, nephrology referral is warranted (NICE, 2015a).
Second trimester
In women with pre-existing diabetes
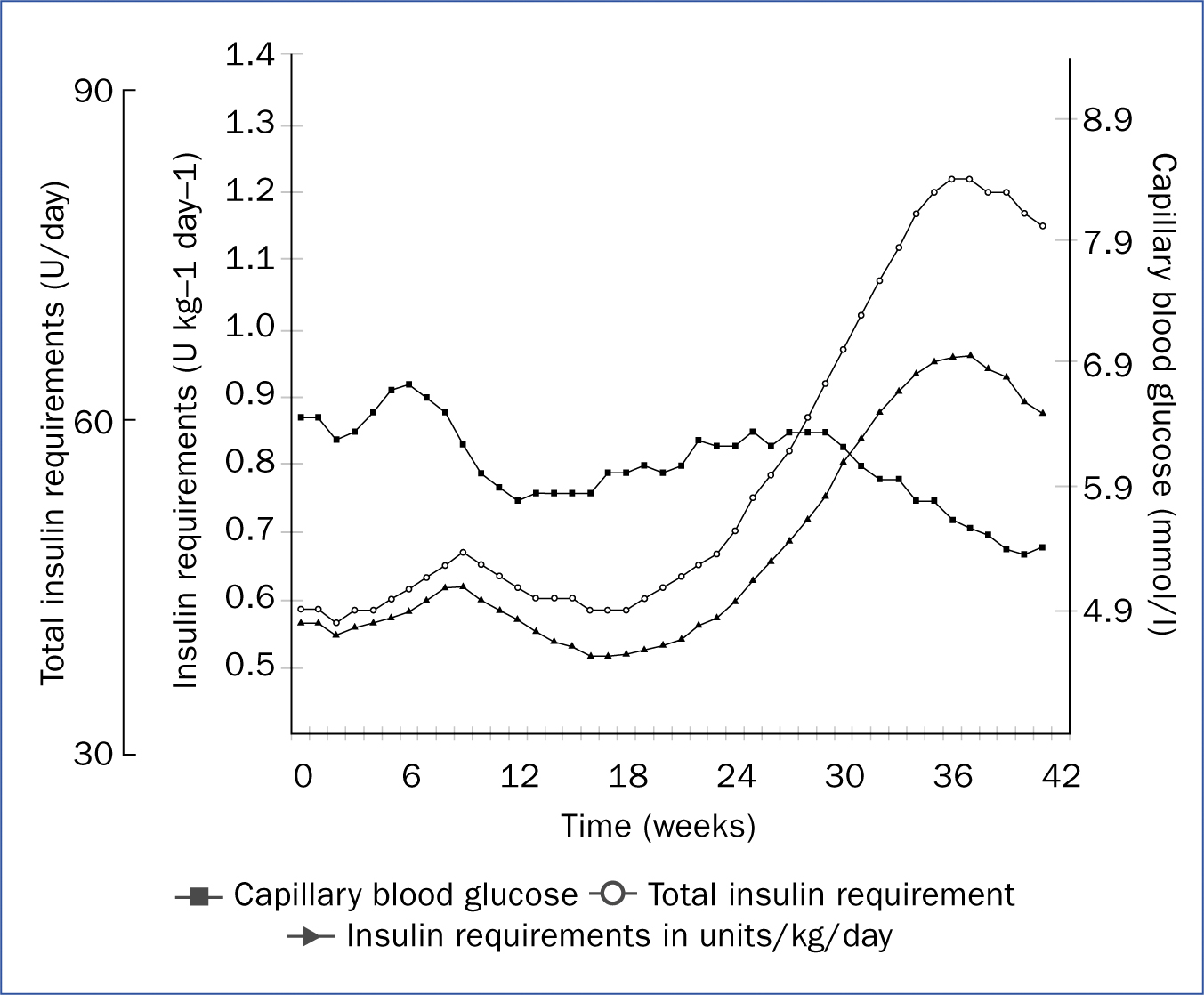
Most women with pre-existing diabetes experience an increase in insulin requirements during the second trimester (García-Patterson et al, 2010; Padmanabhan et al, 2014). This is due to a 50-70% rise in the body's insulin resistance, generated by hormones made by the mother and the placenta (Figure 3) (Catalano et al, 1999; García-Patterson et al, 2010). Ensure that women have a fetal anomaly scan at 20 weeks' (NICE, 2015a).
Third trimester
Insulin requirements vary throughout pregnancy (Figure 3). The emphasis at 28 weeks' is monitoring with ultrasound to assess fetal growth and amniotic fluid volume (NICE, 2015a). Retinal eye screening is needed in the third trimester, as pregnancy can worsen pre-existing eye disease. If polyhydramnios or increased estimated fetal weight is present in women with GDM at any point from 32 weeks', self-monitoring of blood glucose is recommended. The presence of hyperglycaemia (pre-meal ≥5.3 mmol/L and 2-hour post-meal ≥6.4 mmol/L or 1-hour post-meal ≥7.8 mmol/L) means they need referral to a joint antenatal diabetes clinic.
A fetal growth scan is needed at 32 and 36 weeks' with assessment of amniotic fluid volume (NICE, 2015a). Towards the end of the third trimester (36 weeks') is a good time to discuss the mode and date for birth. The mother should also be prepared for the possibility of being on insulin infusion during active labour. Postnatal management, and the likelihood of reduced requirement of insulin and metformin postnatally for mothers with pre-existing diabetes, can also be discussed.
Timing of birth
For women with any form of diabetes in pregnancy, birth after 38 weeks' gestation is associated with greater risk for large-for-gestational-age babies, neonatal death and shoulder dystocia. Therefore induction of labour or caesarean section should be offered if indicated to all women with pre-existing diabetes at 37–38+6 weeks' (NICE, 2015a).
In those with uncomplicated GDM, it can be possible to give birth no later than 40+6 weeks. However, offer induction of labour or caesarean section for women who have not given birth at this time (NICE, 2015a).
A note on the effect of steroids
Steroids are commonly used in the third trimester to aid fetal lung maturation and avoid respiratory distress syndrome in the neonate. They should be given when delivery is planned before 38 weeks' gestation (NICE, 2015b); however, steroids increase blood glucose levels and so an increased insulin dose, or even an insulin infusion, may be required (NICE, 2015a). Therefore, ensure that the diabetes team are involved in the care of women with diabetes who are receiving steroids.
Care during labour
Maternal glucose >10 mmol/L at the time of labour puts the baby at high risk of neonatal hypoglycaemia because of the insulin release in the baby (Brown et al, 1999). Therefore, intravenous insulin is used to maintain normoglycaemia if the woman has been needing insulin or diabetes medication during her pregnancy. The American Diabetes Association (2018) and American College of Obstetricians and Gynaecologists (2017) recommend maintaining levels of 6.1 mmol/L; while the NICE (2015a) and Joint British Diabetes Societies for Inpatient Care (JBDS-IP) (2017) guidelines recommend blood glucose between 4–7 mmol/L. You should therefore refer to your local guidelines.
During the early (latent) phase of labour, the insulin infusion rate is often fairly stable, but during the active phase, insulin requirement can drop markedly. This is because the glucose use by the mother is equivalent to that required during rigorous exercise. The liver's glucose supply (glycogen) is sufficient during the early phase of labour, but during the active phase of labour, the hepatic glucose supply runs out and so calorie supplementation (in the form of intravenous glucose) is required.
Table 1 is a guide for the management of women with pre-existing diabetes and GDM in labour.
| Women with type 1 diabetes | Women with type 2 diabetes | Women with GDM |
|---|---|---|
|
|
|
|
Postnatal care
During breastfeeding, blood glucose levels fall because of high metabolic demand. Women therefore need to take extra calories to maintain blood levels. This particularly applies to mothers with pre-existing diabetes.
In women with pre-existing diabetes, it is important to note that insulin requirements can drop by 30–50% in the first days after birth, so a diabetes team will need to adjust medications. Metformin and glibenclamide can be safely used while breastfeeding.
For women with GDM, all glucose-lowering diabetes medications should be stopped (NICE, 2015a; JBDS-IP, 2017). Post-prandial glucose monitoring should continue for 24 hours after birth. This is done to capture pre-existing diabetes or impaired glucose tolerance (JBDS-IP, 2017). Once the placenta is delivered, the mother's body gradually changes back to its pre-pregnancy glucose-handling ability over the following 1–2 weeks. If pre-meal blood glucose is ≥7 mmol/L and post-meal blood glucose is ≥11.1 mmol/L, the diabetes team needs to be informed (JBDS-IP, 2017). Women should also receive lifestyle advice and have HbA1c or fasting glucose checked at 6–13 weeks postpartum to determine whether diabetes persists after pregnancy (NICE, 2015a; JBDS-IP, 2017). An OGTT is not necessary for all women after pregnancy. Their future risk of GDM will be between 30-84%, depending on ethnicity and body weight.
Conclusion
Awareness of the effect of diabetes on maternal and fetal health is important, due to the increasing numbers of women with diabetes becoming pregnant, and increasing numbers of women developing GDM. Many complications of diabetes in pregnancy can be anticipated and prevented. Knowledge of the management of diabetes in pregnancy, and the early involvement of multidisciplinary team, improve outcomes in these women and their children.