

Prenatal vitamin and minerals supplementation, or hematinics, are essential dur ing pregnancy to promote maternal and child health. The supplements consist of iron (Fe), folic acid, vitamin B12, zinc (Zn), and cobalt (Co). The main function of hematinics is to increase serum erythropoietin level in the blood since the concentration of this serum drops during pregnancy (Hambali et al, 2016).
The common physiological changes that occur during pregnancy include cardiovascular, respiratory, haematological, renal, gastrointestinal and endocrine systems (Tan and Tan, 2013). During pregnancy, the plasma volume increases to approximately around 30–50% (1 200–1 300 ml). The blood volume begins to increase as early as seven weeks of gestation by 10%–15% and the spike occurs at 30–34 weeks of gestation. The red blood cells also increase and this is triggered by an increase in erythropoietin secretion from the kidney. It has been reported that the 18%–25% increment in the red blood cell caused an imbalance towards the 30%–50% increment in the plasma volume, which resulted in anaemia (Tan and Tan, 2013).
The prenatal supplementation programme has been recommended and introduced for pregnant women at an early stage of pregnancy. Oral iron supplementation has been clinically shown prevents iron deficiency (Thirukkanesh and Zahara, 2010) and reduces the risk of birth or fetal defects such as spina bifida, anencephaly, and encephalocele (Hambali et al, 2016). In Malaysia, tablets of ferrous fumarate, folic acid, vitamin B complex and vitamin C are a provision for pregnant women. All pregnant women, regardless of haematological status or trimester, were given oral prophylactic iron, folic acid supplements and both vitamin B complex and vitamin C during their first antenatal care visit until delivery (Ministry of Health Malaysia, 2013). In Malaysia, vitamin and mineral supplementation programmes have been a major strategy to reduce iron deficiency during pregnancy and regular review of the strategy is needed to improve the effectiveness of the programme.
Despite many intervention programmes in reducing the prevalence of anaemia in Malaysia, such as national policies of oral prophylactic supplementation, a health education programme, pre-pregnancy screening and a safe motherhood programme, the disease is still an ongoing issue. About 50% of patients worldwide do not follow the prescribed therapy or treatment. This is a form of non-adherence that gives a huge challenge to the healthcare team (Wilke et al, 2012). Non-adherence usually leads to poor clinical outcomes and will increase the cost for healthcare (Wilke et al, 2012).
Methods
A cross-sectional study was conducted at a maternal and child health clinic in Selangor, Malaysia. A total of 64 pregnant women were selected using a simple, random sampling method. However, a total of 100 respondents were successfully recruited in this study. The inclusion criteria were Malaysian citizen with 18 years old and above, and registered at the maternal and child clinic in Selangor, Malaysia in 2018. Any pregnant women refusing to participate were excluded from this study. This study was conducted from December 2017 until September 2018.
Data collection
The questionnaire used for data collection was a self-guided administered questionnaire, comprised of sections I and II. In section I, the respondent has to answer the sociodemographic information and the determinant factor for non-compliance towards vitamin and mineral supplements. The antenatal data was completed by the researcher based on the antenatal record book at the clinic. In section II, information on the intake of the supplements by the respondents in the past seven days were completed by the researchers by interviewing the respondents to measure compliance percentage. Pregnant women who consumed at least 70% of the expected dose of vitamin and mineral supplements in the past seven days were categorised as compliance.
This questionnaire was adopted from Thirukkanesh and Zahara (2010), and modified accordingly. The modified questionnaire was tested for reliability using inter-rater reliability method (Cohen's kappa coefficient=0.6–1). The result indicates moderate agreement to a very good agreement. It was also pre-tested among pregnant women from the same study site and representing 10% of the sample size. The validity of the questionnaire was performed among five experts in obstetrics and gynaecology. A content validity index (CVI) survey was prepared for the expert to score or rate using Likert scale (1 – not relevant, 2 – slightly relevant, 3 – somewhat relevant, 4 – relevant) for each of the items in the questionnaire. The generated value for Cronbach Alpha was 0.8.
Data analysis
Data were analysed using Statistical Package for Social Science (SPSS) version 23. Descript (mean, percentage and standard deviation) and inferential statistic (Chi-square (x2) test, binary logistic regression) were used for data analysis and p<0.05 is considered statistically significant.
Results
Socio-demographic characteristics of the respondents
Among the 100 respondents, 95% of the CI on the mean age of the respondents is 29.69 years old (28.77–30.61). The minimum age of the respondent was 21 years old while the maximum age was 42 years old. A large number of the respondents were Malay (76%), all of the respondents were married and more than half of the respondents (53%) were employed. Majority of the respondent's (58%) household income was categorised as low income (RM1 000–RM 4000 per month). The respondent's education level was mostly at a tertiary level, which was reported among 64% of the respondents. Nearly three-quarters of the respondents were multiparous (71%) and the remaining were primiparous (29%). Majority of the respondents (49%) were in the third trimester whereas 38% were in the second trimester and 13% were in the first trimester (Table 1).
Table 1. Sociodemographic and antenatal characteristics of the respondents (N=100)
| Characteristics | n (%) |
|---|---|
| Sociodemographic | |
| Age | |
| Mean age (95% CI) | 29.74 (28.85–30.63) |
| Race | |
| Malay | 76 (76) |
| Chinese | 8 (8) |
| Indian | 12 (12) |
| Others(Orang Asli) | 4 (4) |
| Marital status | |
| Married | 100 (100) |
| Occupation | |
| Employed | 53 (53) |
| Self-employed | 12 (12) |
| Unemployed | 35 (35) |
| Household income | |
| ≤RM 4 000 | 58 (58) |
| ≥RM 4 001 | 42 (42) |
| Education | |
| Primary level | 2 (2) |
| Secondary level | 34 (34) |
| Tertiary level | 64 (64) |
| Antenatal Parity | |
| Primiparous | 29 (29) |
| Multiparous | 71 (71) |
| Trimester | |
| First | 13 (13) |
| Second | 38 (38) |
| Third | 49 (49) |
Compliance towards vitamin and mineral supplementation among respondents
According to the self-reported intake of supplementation for the past seven days, 86% of the respondents were compliant towards the supplementation, while only 14% were not compliant (Figure 1). The major factor reported as an obstacle for not complying to the supplementation was forgetfulness (43%), while the main fear of the supplements side effect reported by the respondents was nausea 31 (31%).
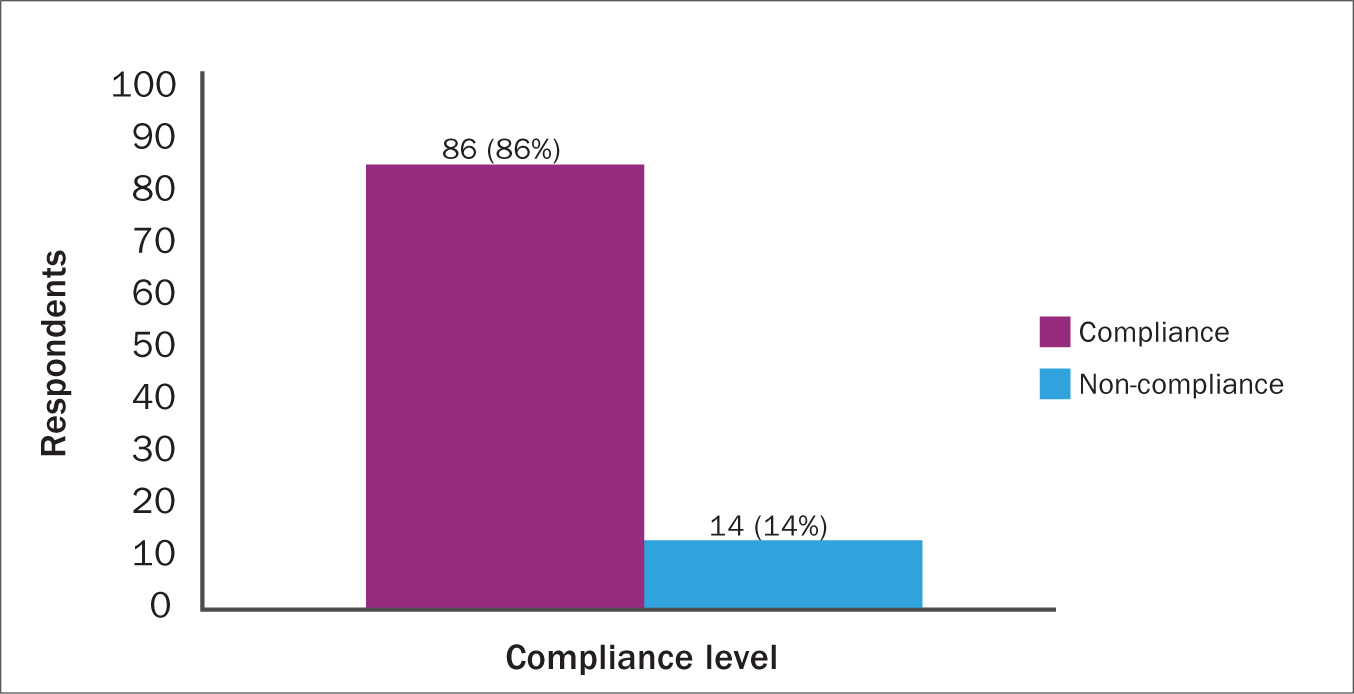 Figure 1. Compliance towards vitamin and mineral supplementation of subjects (N=100)
Figure 1. Compliance towards vitamin and mineral supplementation of subjects (N=100)
Sociodemographic characteristics were significantly associated with the compliance level to vitamin and mineral supplementation among the respondents (p<0.05) except for age (Table 3). They were the contributing or influencing factor that leads to non-compliance to the supplementation. Table 2 shows that younger and older pregnant women have the highest compliant and non-compliant (91%) probability towards the supplements. This data shows that there is no significant association (p>0.05) between sociodemographic characteristic (age) with compliance level.
Table 2: Sociodemographic and antenatal factor influencing compliance (N=100)
| Compliance | x2 | p-value | ||
|---|---|---|---|---|
| Factors | Compliance n (%) | Non-compliance n (%) | ||
| Sociodemographic Race | ||||
| Malay | 69 (69) | 7 (7) | ||
| Chinese | 7 (7) | 1 (1) | 9.494 | 0.02* |
| Indian | 7 (7) | 5 (5) | ||
| Others | 3 (3) | 1 (1) | ||
| Occupation | ||||
| Employed | 51 (51) | 2 (2) | ||
| Self-employed | 10 (10) | 2 (2) | 10.847 | |
| Unemployed | 25 (25) | 10 (10) | <0.01* | |
| Household income | ||||
| ≤RM 4 000 | 46 (46) | 12 (12) | 5.133 | |
| ≥RM 4 001 | 40 (40) | 2 (2) | 0.02* | |
| Education | ||||
| Primary | 2 (2) | 0 | ||
| Secondary | 24 (24) | 7 (10) | 10.226 | |
| Tertiary | 60 (60) | 4 (4) | < 0.01* | |
| Antenatal Parity | ||||
| Primiparous | 23 (23) | 6 (6) | 10.226 | |
| Multiparous | 63 (63) | 8 (8) | ||
| < 0.01* | ||||
| Trimester | ||||
| First | 13 (13) | 0 | ||
| Second | 28 (28) | 10 (10) | 8.290 | 0.02* |
| Third | 45 (45) | 4 (4) | ||
Table 3. Association of determinant factor with compliance to the supplements among respondents (N=100)
| Factors | Compliance n (%) | Non-compliance n (%) | x2 | p-value |
|---|---|---|---|---|
| Severe side effects | ||||
| Yes | 1 (1) | 4 | 19.042 | <0.01* |
| No | 85 (85) | 10 (10) | ||
| Worry to have big baby | ||||
| Yes | 1 (1) | 0 (0) | 0.164 | 0.69 |
| No | 85 (85) | 14 (14) | ||
| Forgetfulness | ||||
| Yes | 35 (35) | 8 (8) | 1.328 | 0.25 |
| No | 51 (51) | 6 (6) | ||
The most significant factor contributing to the non-compliant among the respondents in this study towards the supplement was the side effects (p=<0.01) (Table 3). The side effects of the supplements reported by the respondents were nausea (31%), unpleasant smell of the supplements (27%), vomiting (22%), constipation (19%), heartburn (16%), loss of appetite (11%), other side effects (2%) and diarrhoea (1%) (Figure 2).
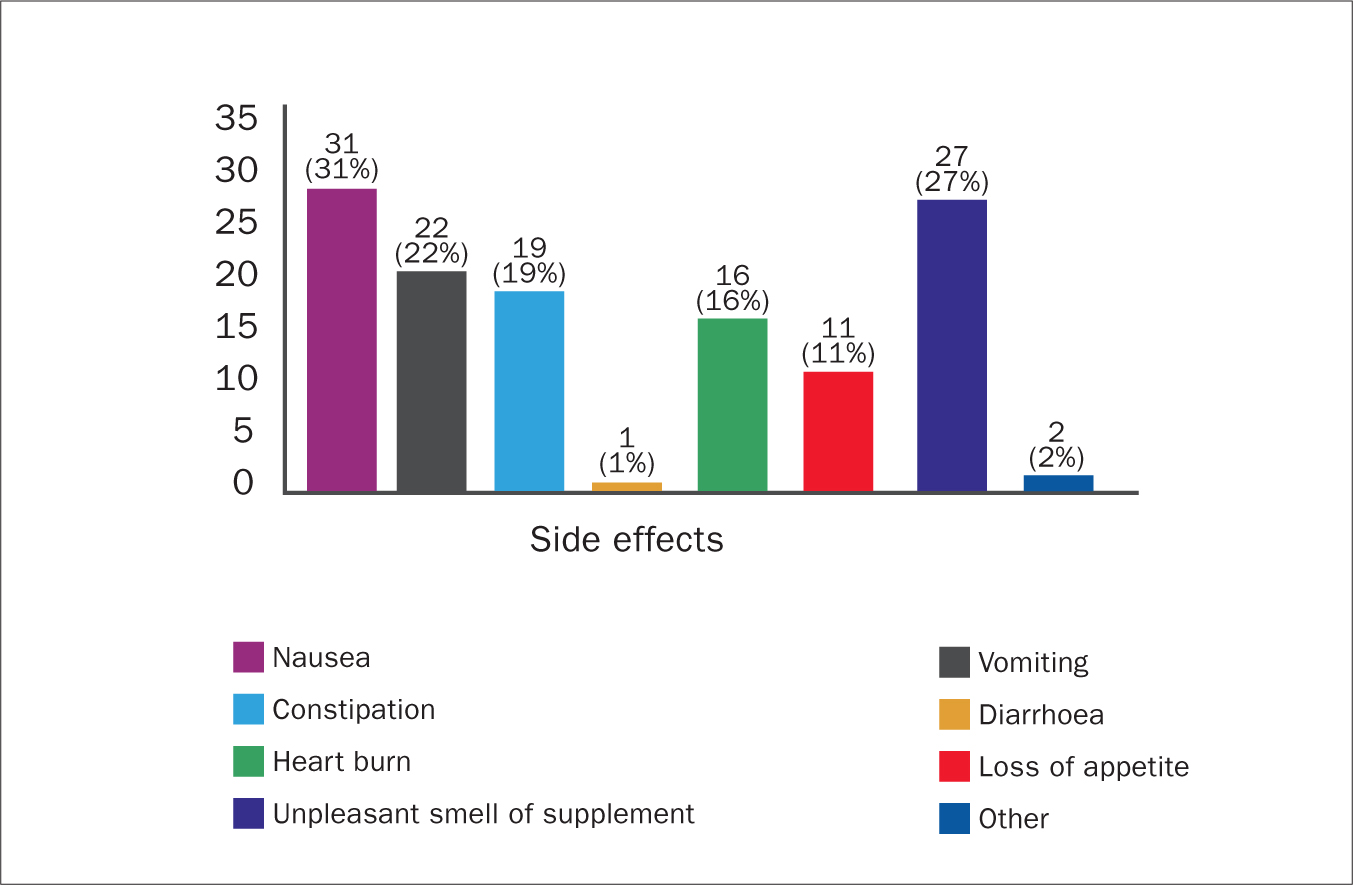 Figure 2. Side effects of vitamin and mineral supplementation among pregnant women
Figure 2. Side effects of vitamin and mineral supplementation among pregnant women
Discussion
Prenatal supplements were suggested for all pregnant women since the main nutrients needed by the body during pregnancy, namely iron and folic acid, are difficult to achieve solely through a food source. This is because, during pregnancy, the women have a higher possibility to develop anaemia due to iron deficiency. Therefore, oral iron supplementation is one of the strategies to reduce the prevalence of anaemia during pregnancy (Sajith et al, 2016). Compliance towards iron supplementation plays an important role in preventing and treating iron-deficiency anaemia, especially the second and the third trimester pregnant women due to the increase in the iron demands (Sajith et al, 2016).
A large number (86%) of the pregnant women in this study were compliant towards the vitamin and mineral supplementation with only 14% of the pregnant women did not comply with the supplementation. The finding of non-compliance in this study is lower than the outcome from a previous study by Thirukkanesh and Zahara (2010). The study reported that half of the pregnant women (50%) did not comply with the supplements prescribed at a maternal and child health clinic in Selangor.
In contrast, a study performed in Ethiopia revealed that 39.2% of the pregnant women were compliant to the supplements (Sadore et al, 2015). Another study in Nepal (Rai et al, 2016) showed a declining number of non-compliance with 73.2% of high compliance, 12.8% of moderate compliance, and 14% of low compliance with the supplementation. These studies thus suggesting that the ratio of non-compliance among pregnant women towards supplementation decrease yearly.
The possible reason for differences between the findings in this study with previous studies may be due to the time gap between the studies and the studied subjects (sociodemographic status). The government has implemented various strategies, such as health education (emphasis on the method of supplements and nutrition intake) and introduction of a new form of prenatal supplementation for pregnant women, to maintain the effectiveness of prenatal supplementation programme (Suzaini et al, 2011). The new form of prenatal supplementation includes Maltofer that is in a form of a chewable tablet and tastes like a sweet. This will reduce the side effects of the supplement and promote compliance among the respondents towards the supplement.
Age and race
Most of the respondent's age were in the reproductive age range which is between 12–49 years old (Medical Dictionary, 2009). Majority of the respondents were Malay (76%), indicating that a higher percentage of Malays utilises the ANC service provided by the public health clinics compared to the Chinese population. This could be due to the majority of Chinese pregnant women prefering to seek treatment at private healthcare clinics since public health clinics have a long waiting time (Yeoh, 2016).
Occupation and household income
All of the respondents were married and more than half (65%) of the respondents were employed, with 35% unemployed. Meanwhile, a large number of the respondents (52%) were in the low middle-income group (RM2 000–RM4 500), more than one quarter (39) were in the high middle-income group (≥RM4 501) and only a small number of respondents (9%) were in the low-income group (RM900–RM2 000).
According to the Department of Statistics Malaysia, based on the survey of the household income of Malaysian's population in 2016, it was reported that 40% were in a low class (B40), 40% in the middle class (M40), and 20% in the higher class (T20) increased in 2016 compared to 2014. The M40 household group has the highest growth with 6.9% per annum followed by B40 group (6.6%) and the T20 group (6.2%). This data showed that majority of the Malaysian population falls within the middle-class group and most of the population prefers to seek medical treatment at public health sector clinics compared to the private sector. A study among pregnant women in France from 2011–2014 found that the most prescribed drug's class was anti-anaemia in 72.5% of those exposed. The study also revealed that more supplementations and vaccines should be channelled to low-income pregnant women (Demailly et al, 2017).
Education
It was recorded that more than half of the respondents (64%) who attended ANC at public health clinic have tertiary education, around one-third of the respondents have secondary education and a small proportion (2%) have primary education. According to the UNESCO Institute of Statistics (2018), the latest data on the level of education among Malaysian population in 2016 reported that 98.9% of nett enrolment rate has a primary education, 73.8% has a secondary education and gross enrolment ratio of 44.1% has tertiary education. This shows that the current trends of the Malaysian population in terms of education level has improved. Majority of the population has at least completed secondary or tertiary education level, such as a university qualification. This is supported by the Malaysian statistic record whereby the percentage of employees completed tertiary education level increased by 1.9%–26.4% in 2014. In contrast, a decrease in the proportion of employees with primary education and no formal education was observed by 1.1% and 0.3%, respectively (Department of Statistics Malaysia, 2015).
Determinant factors of non-compliance
A small number (5%) of the respondents in this study reported that severe side effects were the influencing factor towards the abundance of the supplement. Another study by Thirukkanesh and Zahara (2010) that examines the same parameters revealed a higher percentage (11.9%) of the respondents reported that side effects were the main barrier in consuming the supplements daily. In contrast to both of these studies, 272 (54.4%) of the pregnant women in Mecha acknowledge that side effect was one of the reasons for non-compliance towards iron folate supplement (Taye et al, 2015).
This might be due to the effectiveness of the health education programme and counselling by the healthcare provider at a public health clinic in Malaysia for pregnant women to overcome severe side effects. According to Ugwu et al (2014), side effects can be reduced if the supplements are consumed with a meal; however, this action will reduce the absorption rate by 40% (Thirukkanesh and Zahara, 2010). It is advisable to consume the supplements early in the morning without breakfast to get full absorption of the mineral throughout the body.
Meanwhile, only 1% of the respondents worry that consuming the supplement will lead them to have a ‘big baby’. This concept stems from ancient beliefs but currently they aware that it is a mythical fact.
This is almost similar to the findings reported in another study whereby 5.1% of the respondents have the same view on the size of the baby (Thirukkanesh and Zahara, 2010). A higher percentage (28.4%) was reported in the study in Mecha whereby 142 pregnant women worry about having a big baby due to the prenatal supplements (Taye et al, 2015). This shows that the big difference between the study in Mecha and Malaysia could be due to the different demographic characteristics of the subjects.
In Malaysia, there are a number of health education programmes and nutritional counselling sessions held at the clinic to increase awareness on the benefits of iron supplementation to mother and baby. Gebre, et al (2015) reported that pregnant women who get nutritional counselling were 1.8 times to compliant compared to those who did not receive any counselling, whereas 1.5 times higher for those with knowledge on the benefits of supplements compared to those who do not have the knowledge.
The major influencing factors of compliance among pregnant women was forgetfulness compared to side effects and worry of having a big baby. This could be due to a low self-awareness on the effect of non-compliance towards the supplements. Previous research in Iran reported the same findings in this study in which the main barrier towards adherence to the supplements was forgetfulness (Siabani et al, 2017). Around 69 of the respondents (56.3%) forget to take the supplements daily and this contributes to non-compliance among the respondents (Siabani et al, 2017). This is supported by a previous study with the same demographic area by Thirukkanesh and Zahara in 2010. The main factor influencing the compliance level was forgetfulness and this was self-reported by 33.9% of the respondents.
The findings in this study are supported by another study conducted in Western Amhara, India and Senegal in which forgetfulness was one of the reasons for non-compliance with 9.2%, 9.68% and 17.2% respectively, and self-reported by the respondents (Taye et al, 2015). Less number of pregnant women tend to forget to consume the supplement in the previous finding compared to this study. This could be due to the increase in the percentage of pregnant women being employed.
The main side effect in pregnant women in this study is nausea, followed by unpleasant smell of the supplement. This finding, supported by Thirukkanesh and Zahara, (2010), in Malaysia, 11.9% of pregnant women detailed the reaction of supplementation, for example, nausea, vomiting and constipation are the contributing factors of rebelliousness to supplementation. A study done by Rai et al (2016) discovered the main barriers towards intake of iron and folic acid supplements was due to its side effects, the price being expensive or the supplement not being easily available, demonstrated moderate to low adherence towards supplements. Hence, most of the pregnant women complained that one of the influencing factors that led them to poor adherence of supplementation are due to the side effects of medication, such as nausea, vomiting and constipation. Whereas the perception of how pregnant women perceived the supplement will cause a negative side effect will also lead to their low compliance with supplementation.
Limitation
Majority of the respondents in this study were inducted from pregnant women who were in the third trimester of pregnancy. Therefore, findings on a larger proportion of women who were in the third trimester might give a bigger impact on the distribution of compliance to vitamin and mineral supplementation among the respondents.
Conclusion
This study highlighted the compliance level among pregnant women towards vitamin and mineral supplementation with a good compliance level (86%) compared to the previous study. Forgetfulness is the major contributing factor to abundant of the prenatal supplementation followed by the fear of severe side effects. Therefore, healthcare providers should reiterate the advantages of the prenatal supplements to the pregnant mother during ANC at the clinic. The healthcare provider also needs to focus on giving health education to pregnant women who are employed and have severe side effects from the supplements, since these groups of women have a higher tendency of forgetfulness.
Key points
- Prenatal vitamins and minerals are supplements made for pregnant women to prevent anaemia, low birth weight and any other complication that might impact both mother and baby's health
- Majority of pregnant women in this study were compliant towards the vitamin and mineral supplementation to promote their maternal and fetus health but forgetfulness was reported as one of the reasons their non-compliance towards the supplements
- There is need for continuous awareness of the importance of vitamin and supplement intake to prevent poor pregnancy outcomes
- Healthcare providers should stress the advantages of the prenatal supplements at the antenatal clinic appointments
CPD reflective questions
- What are prenatal vitamins and mineral, and why is it importance during pregnancy?
- List the type of vitamins and minerals needed during pregnancy
- What are the complications associated with vitamin and mineral deficiency in pregnant women and how can it impact the fetus?