
The findings of the Birthplace Study (Birthplace in England Collaborative Group, 2011) should have resulted in a significant increase in the numbers of low-risk women giving birth either at home or in alongside and free-standing birth centres (Boseley, 2011; Rogers et al, 2012; Warwick, 2012). If the percentage of home births is a barometer for the number of women giving birth outside obstetric units, then sadly we are adrift and the findings have not been translated into practice. Data from the Office for National Statistics (2013) showed a continuing decrease in the percentage of homebirths from 2.4% in 2011 to 2.3% in 2012. According to data published by National Institute for Health and Care Excellence (NICE, 2014), 90% of women giving birth in the UK continue to do so in designated consultant/consultant GP units. This leads to the question of why so many women continue to choose to give birth in a consultant unit considering the evidence (Birthplace in England Collaborative Group, 2011). Compare this with women's decision-making following the publication of the Hannah et al's (2000) term breech trial (Lawson, 2012). The less favourable outcomes for babies of women having vaginal breech deliveries resulted in an immediate change in the management of breech births. It is inconceivable why the Birthplace Study did not lead to a similar response given the significantly increased serious morbidity for low-risk mothers planning birth in an obstetric unit. Nevertheless, Rogers et al (2012) argued that translating the Birthplace findings into practice would present challenges given the deeply entrenched belief among women and professionals that birth in obstetric units was safest. To address this, Rogers et al (2012) argued that maternity providers and commissioners would need to develop a robust strategy with strong leadership to drive the realisation of the evidence. The purpose of this paper is to present a strategy and experience of encouraging low-risk women to plan to give birth in a midwife-led setting.
At the time of the publication of the Birthplace Study, the Royal Free London NHS Foundation Trust provided maternity services for approximately 6700 women per year. Women who met the midwifery-led criteria could choose to give birth at home, in the free-standing birth centre, in one of two alongside midwifery-led units or on either of the two consultant-led delivery suites. However, only 15% of all women booked birthed in the midwifery-led settings (Rogers et al, 2012). It was believed that the long-awaited findings of the Birthplace Study (Birthplace in England Collaborative Group, 2011) provided the evidence that would enable a change in the direction of planned place of birth for low-risk women locally. The aim was for 30% of local women to give birth outside the Consultant Obstetric Unit by 2014 (Rogers et al, 2012). The responsibility for developing and leading the change was devolved to the local midwifery-led management group led by the consultant midwife. As part of this process, the factors that influence women's choice and strategies to better enable informed choice were reviewed.
Choice of planned place of birth
Although there has been a number of studies investigating women's perception of the birth place choices offered (Garcia et al, 2006; Redshaw et al, 2007; Healthcare Commission, 2008; Care Quality Commission, 2010), there is a paucity of literature examining the factors that influence a woman's choice (Barber et al, 2006a; Barber et al, 2006b; Houghton et al 2008). Barber et al (2006a and b) found that both the woman's personal beliefs and those of her partner were the main factors that influenced birthplace choice. Their beliefs with regard to the safety of the different options offered were of particular importance, with women perceiving hospital births as safest. Barber et al's (2006a and b) findings were similar to those of Houghton et al (2008) who reported that the perceived increased safety and security of hospital births was the main reason why women choose that option.
The study by Houghton et al (2008) provided an in-depth exposition of women's rationale for choosing hospital births. Women in this study spoke of the ‘risks’ of out-of-hospital births and possible complications if immediate access to medical support and resources were not available. For many women the possibility of giving birth outside an obstetric unit was not within their conceptual framework as they not only believed hospital birth to be safer but believed they were expected to give birth there. Other alternatives were perceived ‘foreign’ (Houghton et al, 2008). In this study, maintaining the ‘status quo’ was important and women choosing alternative birth settings were seen as ‘different’. Participants in the study believed that intervention in childbirth was the norm and thus accepted as part of the birth process. According to the authors, a ‘lack of faith in birth without intervention undermined consideration of birthplace options other than a full equipped hospital’ (Houghton et al, 2008). This belief was borne out in the experience of women studied as many experienced complications and interventions. In contrast to the findings of the Birthplace Study, women in this study did not perceive the intervention to be associated with the birth setting, for most it was perceived as a necessary part of the birthing process. Another important factor influencing women's choices is the way these options are offered, with a number of studies showing information presented is often biased to promoting hospital birth (Levy, 2004; Pilley-Edwards, 2004; Rogers, 2009). The studies show that professionals can be deliberately coercive with the promise of a healthy baby because they themselves believe the safest place to give birth is in a hospital environment (Levy, 2004; Pilley-Edwards, 2004; Rogers, 2009).
Professionals’ attitudes and beliefs have been shown to have a significant impact on women's choices. Houghton et al (2008) reported that midwives viewed hospital births as protecting the women. Births outside hospital were viewed as being ‘inferior’ in terms of safety. As with the women in Houghton et al's (2008) study, professionals felt more confident in hospital birth and believed it to be the safest environment. The study also highlighted that health professionals felt it was the woman's responsibility to request alternative birth settings and was not for them to routinely offer these choices. Ironically, women were concerned about requesting alternative birth settings because of their perceptions of the response from health professionals (Houghton et al, 2008). The study by Mead and Kornbrott (2004) confirmed the interconnected relationship between the experience of midwives and their perception of birth outside obstetric units. The study found midwives working in obstetric units with high rates of intervention had a significantly higher perception of risk than midwives working in units with lower intervention rates. The study also reported that midwives overestimated the advantages of interventions and underestimated the woman's ability to have a normal birth. To date there is limited evidence exploring midwives’ views on place of birth but there is a consensus in the literature that it is difficult for midwives to promote choice and facilitate birth outside obstetric units if they have limited or no experience of supporting women in these settings (Houghton, 2008; McCourt et al, 2012; Warwick, 2012).
The evidence confirmed that deeply embedded concerns among women and midwives over the safety of birth outside consultant units required a coordinated, multi-faceted approach if the vision of 30% of local women to give birth outside the Consultant Obstetric Unit by 2014 was to be realised. The main themes to be addressed were the promotion of informed choice and midwives’ knowledge and confidence in promoting birth outside obstetric units.
Strategies focusing on women and their partners
In order to address women's concerns about the safety of birth outside consultant-led units and to consider the quality of information given to enable women to make an informed choice, a number of innovations were prioritised, including:
The purpose of these combined strategies was to ensure that all women using the Trust's services had access to the correct information to enable them to make an informed choice on planned place of birth.
Birthplace workshop
The aim of the workshop was to promote facilitated group interaction and discussion around birthplace choices, including the reasons, evidence and different options.
Given women's beliefs and perception around the increased safety of hospital births, disseminating and discussing the findings of the Birthplace Study was a key focus of the workshop. All low-risk women and their birthing partners were invited to attend these workshops at around 24 weeks’ gestation. The workshop was facilitated by an experienced midwife conversant in the findings of the Birthplace Study and women's fears of giving birth in alternative birth settings. The aims of the workshop were:
During the workshop women and their partners were given the opportunity to explore in small groups the advantages and disadvantages of giving birth either at home, at the alongside midwifery-led unit, at the Trust's free-standing unit or on a consultant delivery suite. Each group was given the opportunity to feedback to the larger group. The facilitator used the evidence from the Birthplace Study to respond to the feedback given.
Decision aids
To promote consistent evidenced-based information, ‘decision aids’ were developed including a poster and an evidence-based discussion tool. The Cochrane collaboration (O'Connor et al, 2009) defined decision aids as interventions designed to help people make specific and deliberate choices by providing information on the options and outcomes relevant to the individual. The review reported that the use of decision aids was superior to usual care interventions in improving knowledge and sharing realistic expectations of the benefits and harms of different options, as well as reducing decisional conflict. The development of the decision aid took approximately 6 months and the team responsible comprised maternity service users, midwives and lead obstetricians of the midwifery-led management group. The decision aid incorporated the findings of the Birthplace Study, outlining both the benefits and drawbacks of planned birth outside the obstetric unit. The decision aid was incorporated into the handheld maternity records and used at booking by the midwife to inform the discussion on place of birth. At every midwifery contact the intention was that the midwife would use the decision aid to review with the woman her intentions about planned place of birth. In this way, the decision aid served two purposes: improving women's knowledge and confidence and improving midwives’ and other health professionals’ knowledge of the study findings.
Review of the maternity service website
The Trust's maternity services website underwent a major review incorporating a virtual tour of our entire midwifery-led services, plus an overview of the Birthplace Study findings including hyperlinks for more information. Stories from women and their partners were included, sharing their experiences and rationales for their birthplace choices. To complement the above strategies and further promote our midwifery-led services, all women and their partners were offered an early pregnancy booking appointment in a midwife-led setting.
Strategies focusing on midwives
It was important to acknowledge the difficulties experienced by midwives and other health professionals of assimilating new evidence that discredits deeply held beliefs. Midwives are the professionals with most influence on a woman's choice of place of birth (Barber et al, 2006a; Barber et al, 2006b; Houghton, 2008); therefore, it was imperative that the Trust's midwifery workforce was aware of the findings and were able to confidently use these to inform their practice. Cognisant of the fact that the majority of the Trust's midwives had limited experience in providing intrapartum care either at home or in the birth centres, it was recognised that enabling and facilitating staff to gain this experience was critical. A series of workshops was facilitated to meet two objectives: to disseminate and promote understanding of the study findings and to identify local requirements for implementing the findings. The aims of these workshops were:
Midwives were shocked by the findings, particularly in view of recent media coverage of the study, which focused on the risks of home birth for first-time mothers and largely ignored the other key findings (Jeffreys, 2011). Midwives were not surprised that women choosing to birth in hospital were likely to experience greater intervention, but they failed to appreciate the nature and severity of the intervention alluded to in the press. The significant differences in the rate of emergency caesarean section and instrumental births were of particular concern. Midwives were given the opportunity to explore the implications of the study for women, for themselves and for the service configuration. Midwives acknowledged the difficulties in promoting choice of birth settings when there was widespread belief that the safest place to give birth was in an obstetric unit. It was believed that the perceived safety of hospital births was the primary reason for the poor uptake of alternative birthplace choices. For many midwives this raised a moral dilemma of offering choice when there was concern about the safety of the choices been offered. As with the findings of McCourt et al (2012), midwives were concerned about their own confidence and experience of supporting women at home or in alternative birth settings as the majority had no experience in this area. To support midwives in strengthening their confidence, workshops focusing on normal birth and caring for women in different birth settings were organised. In addition, where possible, the on-call rota comprised midwives with different level of experiences in order to ensure that there was always an experienced senior midwife available for advice and support.
Monthly audit reports were collated; these included numbers of women booking to give birth outside the consultant unit, outcomes for women labouring outside consultant units, the percentage of women eligible at booking to give birth in a midwife-led setting as well as reasons identified at booking for women wanting to give birth in an obstetric unit. The use of the decision aid was also audited as was the uptake and experience of women attending the Birthplace workshop. Providing feedback was essential to maintain the motivation of staff and to embed the changes in practice. While it is difficult to quantify the contribution of any of these strategies, it is believed that this work has improved choice for women and begun to translate the findings of the Birthplace Study into practice.
Impact on practice
In the most recent Pickers survey (2013): 97% of women reported having been given a choice of where to have their baby, compared with 93% in previous reports. Nevertheless, 45% of women still reported that they had not received enough information to help them make an informed choice. However, across London, women who gave birth at the Trust reported being more likely to have been offered a choice of place of birth and less likely to report having received insufficient information on which to base their choice (Rogers, unpublished).
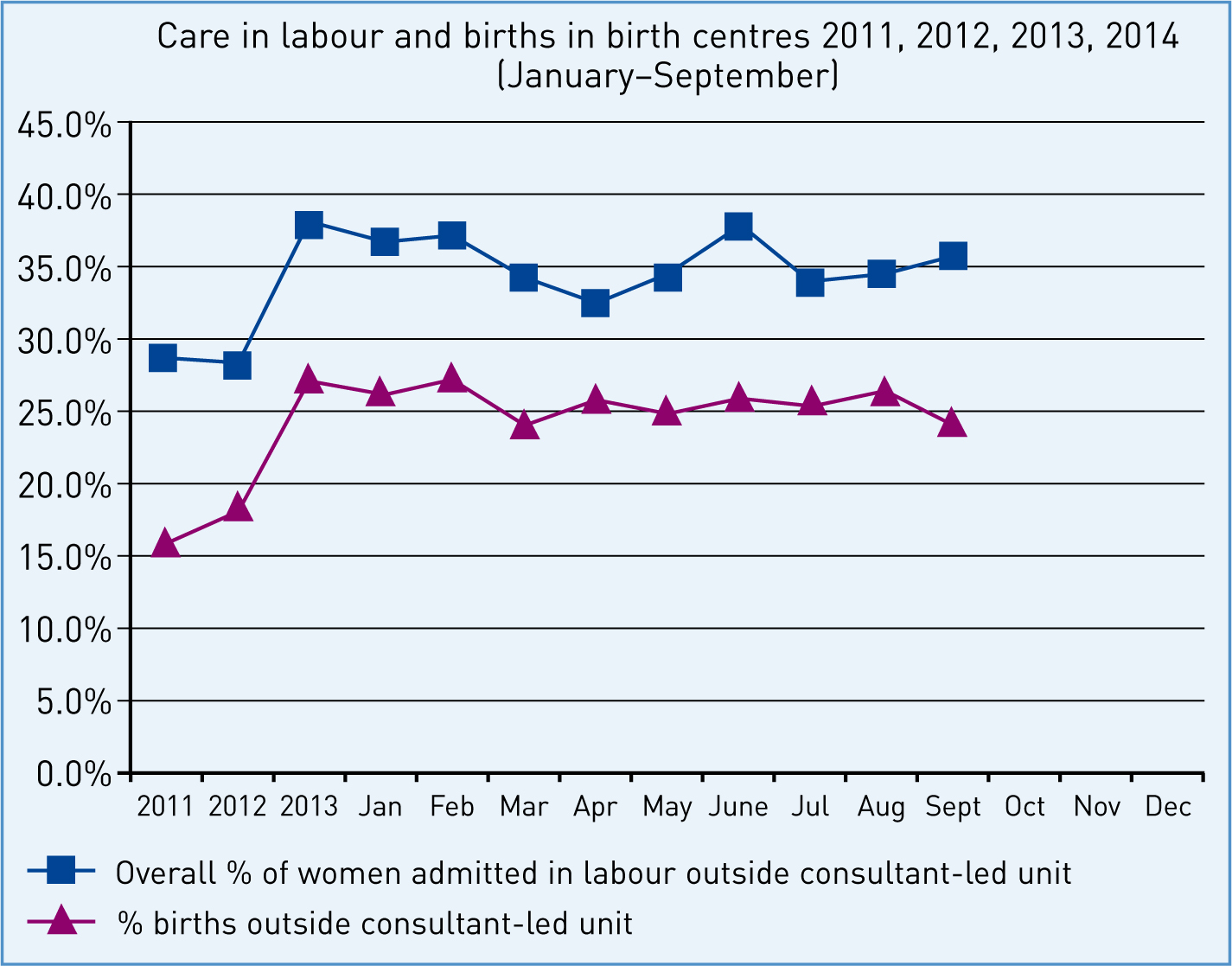
Figure 1 provides comparative data on the percentage of women labouring and birthing in the Trust's free-standing or alongside birth centres for the period 2011 to September 2014. Overall, admissions and births have increased by more than 10% to date.
The Birthplace Study (Birthplace in England Collaborative Group, 2011) reported that 4.4% of low-risk women planning to give birth outside an obstetric unit had an emergency caesarean section, compared to 11.5% for women planning birth in an obstetric unit. The results of this study were similar to those of the Birthplace Study, with less than 4% of women delivered by emergency caesarean section (Table 1).
| Mode of birth | n | % |
|---|---|---|
| Normal delivery on birth centre | 1203 | 82.39 |
| Spontaneous vaginal delivery on labour ward | 107 | 7.32 |
| Instrumental | 98 | 6.71 |
| Emergency caesarean section | 52 | 3.56 |
| Total | 1460 | 100 |
Women meeting the criteria for midwifery-led birth could have chosen to give birth at home in an alongside birth centre or in a free-standing unit (Table 2—data for 2014 is for 9 months only). Overall, Table 2 shows the percentage of women giving birth in the Trust's alongside units has increased, the percentage of women giving birth at home has remained relatively unchanged at around 5%; however, the percentage of women birthing in the free-standing units has significantly decreased from approximately 23% in 2010 to 9% for the first 9 months of 2014.
| 2010 | 2011 | 2012 | 2013 | 2014 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Place of birth | n | % | n | % | n | % | n | % | n | % |
| Alongside unit | 859 | 71.40 | 771 | 68.65 | 1000 | 74.62 | 1107 | 78.23 | 778 | 86.44 |
| Free-standing birth centre | 273 | 22.69 | 267 | 23.77 | 260 | 19.40 | 227 | 16.04 | 79 | 8.70 |
| Home | 71 | 5.90 | 85 | 7.56 | 80 | 5.97 | 81 | 5.72 | 43 | 4.77 |
| Total | 1203 | 1123 | 1340 | 1415 | 900 | |||||
Discussion
The NHS Mandate, 2014 reaffirms the government's commitment to promoting choice for women (Department of Health (DH), 2014). The results of this study highlight the importance of multi-faceted interventions to improve the quality of information to women to enable them to make an informed choice about planned place of birth as well as to encourage them to plan to give birth outside an obstetric unit. Data for 2014 show that about 35% of women planned to give birth in midwifery-led birth settings with more than 25% of women achieving this aim. Across London, the Royal Free London NHS Foundation Trust has the highest number of women choosing midwifery-led birth settings and this study is being used to inform the work of the strategic clinical network (Read, 2014). Nevertheless, there is no room for complacency given the low numbers of women choosing to give birth at home and the decrease in women birthing in the free-standing unit. This is disappointing, but may be part attributable to the withdrawal of a 24-hour dedicated midwifery team, the opening of a new alongside midwifery unit, and the confidence of the community midwives providing intrapartum care in the home or in a standalone birth centre. Addressing the community midwifery confidence and experience is a key priority. The importance of appropriate models of care to enable midwives to develop skills and confidence in different birth settings cannot be underestimated (McCourt et al, 2012). In the Trust, community midwives provide antenatal and community care and an on-call service for women birthing at home or in the midwifery-led settings supported by a small core of dedicated staff in the birth centres. The Trust aims to have a senior midwife (Band 7) on duty in the midwifery-led units 24/7 to support and lead standards of care for women in these settings. This is critical for ensuring safety and for supporting the development and confidence of staff caring for women in labour. Furthermore, the Trust now endeavours to have an experienced, confident, first on-call midwife for women planning to give birth at home or in the free-standing birth centre. Bespoke workshops for all staff providing care in these settings have been launched. Experience, to date, suggests that a variety of models may be required to enable the most effective implementation of the Birthplace Study findings. Work continues to enable the identification of the most appropriate model or models locally. The importance of addressing community midwifery competence and confidence in providing care in these settings is highlighted by the updated Intrapartum Guidelines (NICE, 2014).
Translating the Birthplace findings into practice has been very challenging despite the commitment, motivation and hard work of the team locally. This has necessitated a major change in the culture that underpins current maternity service provision as well as the professionals providing care, but more importantly, women and their families accessing care. Culture, in this sense, refers to deeply entrenched values and beliefs that define how services are organised and the choices offered and selected. Despite the current rhetoric of informed choice, the increasing medicalisation of childbirth has had a major impact on the provision of care and attitudes towards birth and safety. According to Schein (2010), organisational culture takes many years to change and requires not only a systematic approach but dynamic leaders and expert practitioners with an in-depth understanding of the change management process as well as the evidence supporting the need for change. The requirement for strong leaders to effect change is well documented in the literature (Royal College of Obstetricians and Gynaecologists et al, 2007, The King's Fund, 2008; Schein, 2010; DH, 2012). Implementing the findings of the Birthplace Study requires investment in midwifery leaders with the knowledge, expertise and credibility to direct the cultural shift required. This project has shown that affecting this cultural shift is arduous, requiring significant investment at organisational level to address the deeply entrenched cultural beliefs that maintain the status quo. Changing perceptions about the safety of different birthplace settings is a critical first step in achieving the overall shift required. The consultant midwife is ideally placed to enable this cultural shift and to lead the development of a midwifery workforce that feels supported and confident to provide safe care in alternative birth settings.
Despite the findings of the Birthplace Study (Birthplace in England Collaborative Group, 2011) and the more recent publications from this study confirming the benefits to women, babies (Rowe et al, 2014; Hollowell et al 2014; Li et al, 2014; Lukasse et al, 2014), progress with the implementation of the findings have been extremely modest. Sandell (2014) maintains that approximately 45% of women are low-risk at the end of their pregnancy and therefore eligible to give birth in a midwifery-led setting: thus maintaining the status quo is no longer an option. It is not acceptable that so many eligible women are not benefiting from the findings of the Birthplace Study. This should no longer be just about choice but about what needs to be done to make midwifery-led birth settings the choice for low-risk women. This has to be the priority if we want to achieve the best outcomes for women and their babies in addition to providing for a cost-effective maternity service. Given the determination to address the budget shortfall in the NHS (Stephens, 2010), normalising birth and reducing intervention, would provide considerable cost savings for any individual Trust. While local initiatives like those presented here are to be commended, these need to be supported by a national campaign and strategy if we are to bring about the required cultural shift and overcome barriers to change. The recommendation in the recently published Intrapartum guidelines (NICE, 2014) advising all low-risk women to have their baby at home or in a midwifery-led unit should provide additional momentum both locally and nationally to translate the findings of the Birthplace Study into practice. It is critical that commissioners, providers, policy makers, professional organisations and women rise to that challenge.
Conclusion
This project has demonstrated the benefit of multi-faceted innovations to enable women and their partners to make an informed choice with respect to place of birth. There has been a significant increase in low-risk women choosing to give birth outside the Trust's consultant unit since the commencement of the project. As well as the benefit to women, the project has raised the profile of midwives within the organisation and with commissioners by reaffirming the contribution of midwives in the provision of a cost-effective and a high-quality maternity service. Nevertheless our experience of implementing the Birthplace findings has shown that, in order to truly reverse the tide and translate the NICE 2014 guidance into practice, a national strategy is required.