
Breastfeeding is a worldwide public health issue, which has a major impact on reducing child mortality and several long-term non-communicable diseases, such as high blood pressure, diabetes and cancer (World Health Organization (WHO), 2013; 2014). In 2010, in the UK 17% of infants were exclusively breastfed at 3 months of age (McAndrew et al, 2012). This figure is far lower than in other European countries, such as Norway with 70% of infants exclusively breastfed at 3 months and Sweden with 60% at 4 months of age. The UK's rates are also lower than other developed countries including New Zealand and Canada (Save the Children, 2012). In terms of women's and children's health, the UK is ranked 10th and 16th, respectively, of 44 developed countries, again being beaten by many of the Nordic countries (Save the Children, 2012). Various strategies have been implemented in the UK to increase breastfeeding rates and duration, such as adopting the International Code of Marketing of Breast-milk Substitutes (WHO, 1981) into law, postnatal breastfeeding support and peer support groups with varying success rates (Brady, 2012; National Institute for Heath and Care Excellence (NICE), 2013). Newer approaches to encourage breastfeeding practices include financial incentives, longer paternity leave and workplace policies for breastfeeding women when returning to work (Whelan et al, 2014; WHO, 2014). However, these strategies face many criticisms and challenges, especially in terms of ethical considerations; nevertheless, breastfeeding rates must increase in line with our European counterparts to improve the health of the nation. Baby Friendly Initiative (BFI) is a leading international programme providing guidance for health care institutions on how to implement best breastfeeding practice, but only 17% of hospitals in the UK have achieved BFI accreditation (Save the Children, 2012; UNICEF UK, 2012). The Government, policy-makers and health-care agencies must try to combat these challenges and implement strategies to support the maintenance of breastfeeding following BFI and WHO standards (UNICEF UK, 2012; WHO, 2014).
The International Code was introduced in 1981 banning the advertisement of breastmilk substitutes to pregnant women, mothers or members of their families (WHO, 1981), with the aim of reducing child mortality and morbidity by preventing individuals to be swayed to artificially feed their babies by media advertising (Brady, 2012). However, currently in the UK, companies can still advertise follow-on formula as manufacturers argued these were not breastmilk substitutes and therefore were not included in the legislation. Many people argue this is still indirectly advertising the use of breastmilk substitutes and therefore should be banned (UNICEF UK, 2013). Researchers in Australia back this having found women perceived toddler milk advertisements to be promoting all artificial formula milks available from birth (Berry et al, 2010). It is challenging for the Government to control company advertising because of the loopholes in the International Code; however, policies must be regularly reviewed and updated to ensure the UK abides by international recommendations (WHO, 1981; Brady, 2012). Health professionals and members of the public can help by reporting any ambiguous or misleading commercial advertisements to the advertising standards authority (UNICEF UK, 2013).
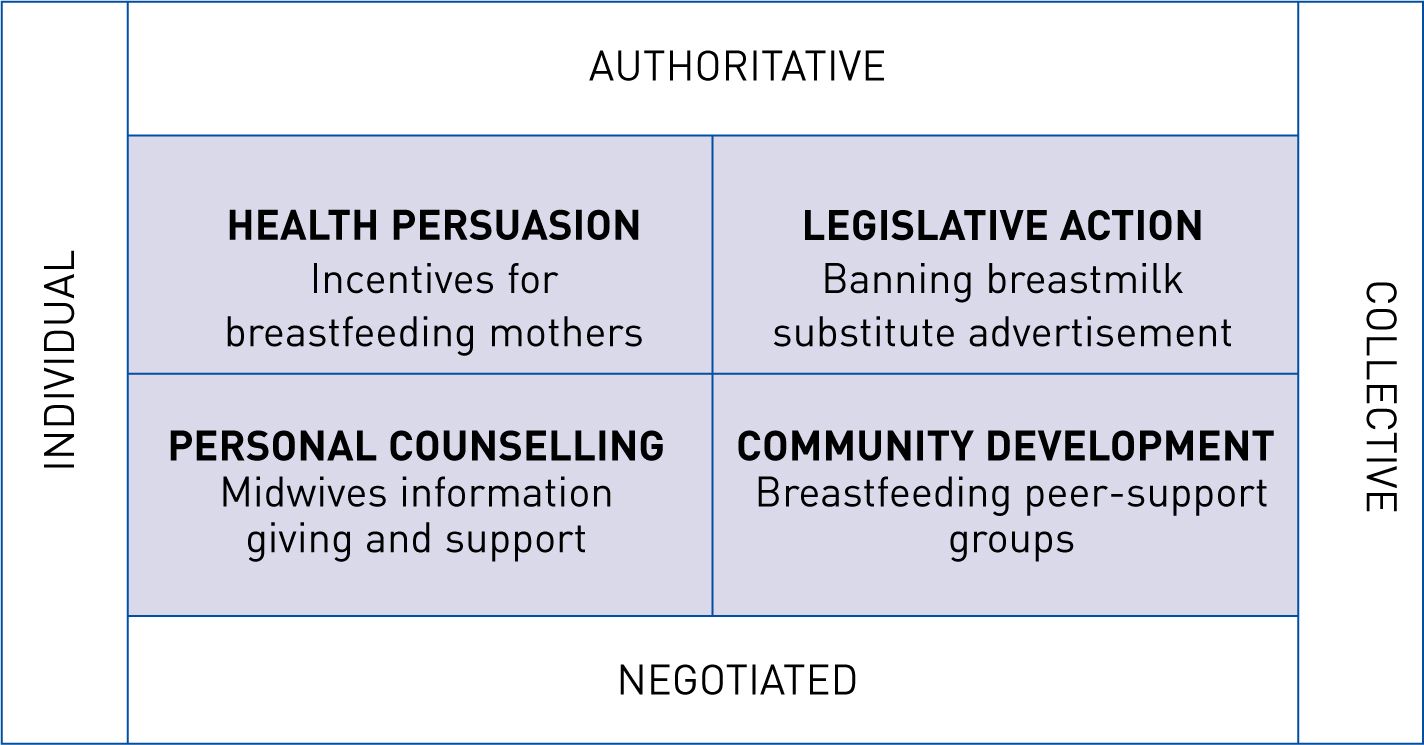
Eliminating advertisements of breastmilk substitutes matches the ‘authoritative collective’ category of Beattie's health promotion model as a legislative action to prevent a collective society from artificially feeding their children (Figure 1) (Thompson, 2014). Some argue that it is beneficial to have an authoritative stance as some argue it has higher rates of success, which is important when public funding is limited and outcomes are important. However, others state that a top-down approach is a less-effective health promotional method as it disempowers individuals and contradicts advice from the Marmot review (2010) that suggests individuals should have control over their life choices (Thompson, 2014).
Paternity leave
Statistics show that Iceland has one of the best breastfeeding rates, with 98% of women in Iceland having breastfed at some stage (UNICEF UK, 2012), but has poor compliance with the International Code and BFI accreditation, which demonstrates how authoritative approaches are not always effective by themselves (Save the Children, 2012). One theory behind Iceland's success is the 13 weeks paternity leave offered to fathers, which has been in place since 2003, a time when the UK's paternity leave increased to 2 weeks (Thorisdotti et al, 2012; The Guardian, 2013). Swedish research found that infants whose fathers did not take paternity leave were significantly less likely to breastfeed at 2, 4 and 6 months of age (Flacking et al, 2010). Sweden and Norway both have a charitable paternity leave of 10 and 12 weeks, respectively, and are praised for their breastfeeding practices (Chalabi, 2013). Flacking et al (2010) suggest that longer paternity leave may lead to increased breastfeeding rates because partners are aware that they have time to develop a relationship with their child, so may not feel that they are missing opportunities to bond when the mother is breastfeeding. Other research suggests that some mothers whose partner's take longer paternity leave feel better, physically and emotionally, at 3 months which could also lead to prolonged breastfeeding rates (Redshaw and Henderson, 2013). In practice, a combination of legislative approaches may be used to promote breastfeeding and the importance of paternity leave must not be overlooked. Paternity leave in the UK has recently been reviewed and updated to include shared parental leave, a scheme whereby the mother and partner can share the 52 weeks' maternity leave between them both (Gov. UK, 2015). This may well be an effective public health measure to increase breastfeeding rates of longer durations, so research should be undertaken to audit the effects of this scheme.
Financial incentives
Another type of health promotion is demonstrated by the introduction of financial incentives for breastfeeding mothers, which theorists may describe as a socioeconomic, health persuasion technique (Figure 1) (Thompson, 2014). Preliminary studies in the UK, Canada and the US suggest that providing financial incentives to breastfeeding women could increase the rates and duration of breastfeeding, but many health professionals are still undecided on whether this scheme is ethically acceptable to roll-out (Relton et al, 2014; Whelan et al, 2014). Crossland et al (2015) argue that as breastfeeding is cost-free, financial incentives could be spent on other poor health choices such as smoking and alcohol consumption. However, if this is successful and breastfeeding rates increase enough for it to become the social ‘norm’, then this public health measure could be a short-term strategy, leading to long-term health benefits; an ideal, cost-effective public health strategy (Whelan et al, 2014). There are ethical implications to consider; these incentives could lead to women feeling guilty if they cannot breastfeed, or do not want to breastfeed (Whelan et al, 2014). However, a utilitarian approach would suggest it is ethical to offer incentives as the consequences would benefit the majority (Thompson, 2010). In practice, more research on the logistics of providing financial incentives to promote breastfeeding in the UK, including which health professional is best suited to validate participants, must be carried out. Policy-makers should investigate what type of incentive would work best—for example, nappies, maternity clothes or breast pumps may be better than cash or shopping vouchers as they ensure incentives are functional and are indeed promoting healthy behaviours (Crossland et al, 2015).
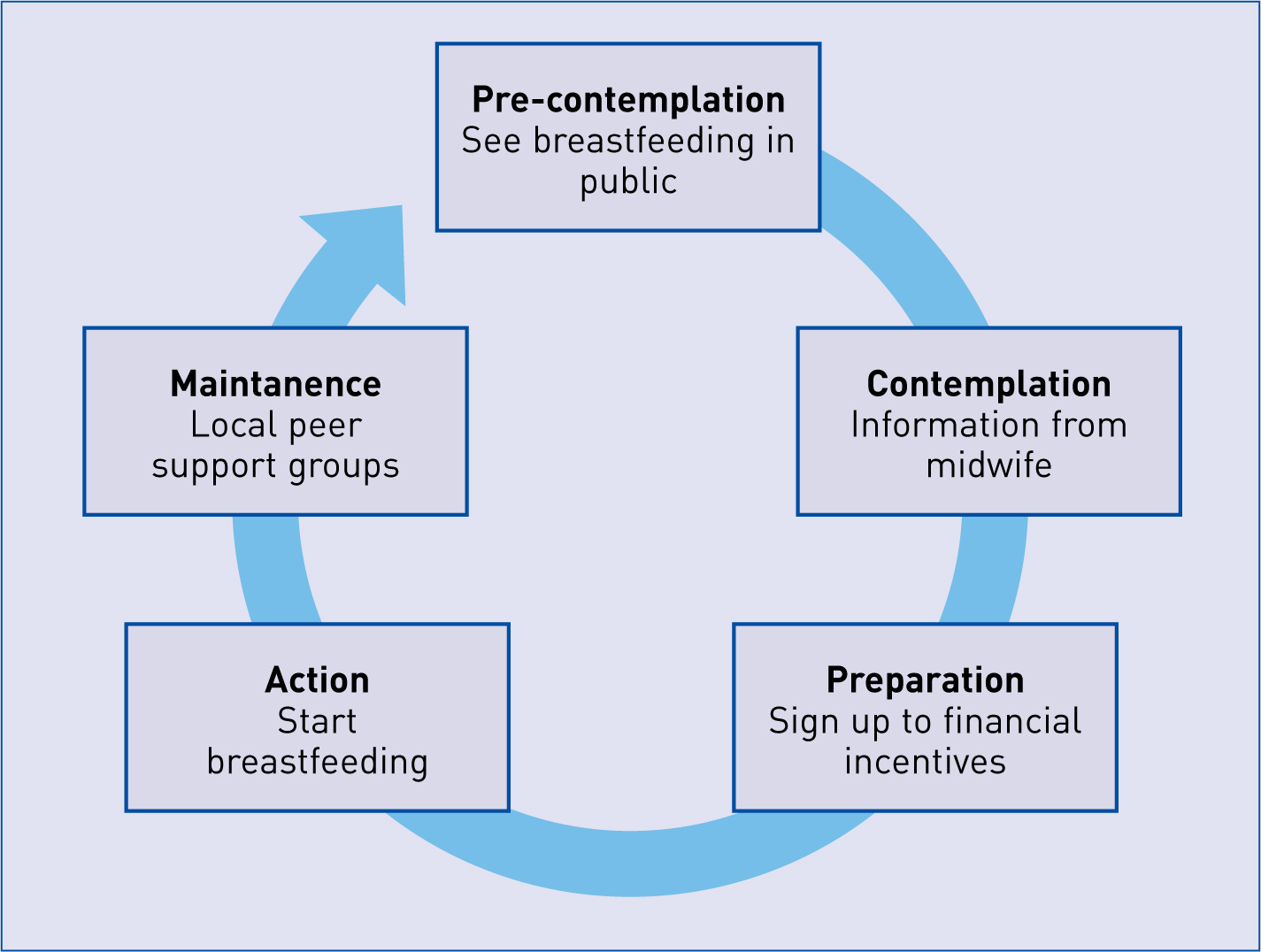
Providing financial incentives to women who breastfeed may encourage them to initially breastfeed, but for women to sustain breastfeeding practices, theorists suggest further actions need to be taken (Thompson, 2014). This is demonstrated by the transtheoretical model (Figure 2), which matches Beattie's health promotion model well, acknowledging that change is an ongoing process, necessitating a wide range of interventions (Thompson, 2014). Research in practice supports this model by demonstrating how postnatal support can help women overcome breastfeeding challenges, therefore prolonging breastfeeding practices (Wen et al, 2011; McLelland et al, 2015). In reality, postnatal visits may be limited in the UK due to funding issues, leading to a significant lack in breastfeeding support, despite of NICE (2013) guidance recommending that clinical commissioning groups increase spending to expand breastfeeding services (Walsh, 2011). As a result, midwives must often refer women to local community peer-support networks, to offer the guidance and reassurance that may be lacking in routine postnatal maternity care, to encourage them to maintain their breastfeeding practices. All multidisciplinary professionals should make every contact count to encourage breastfeeding maintenance; for example, nurses during infant immunisation appointments and health visitors during routine appointments (Department of Health, 2012; Elliott-Rudder et al, 2013).
Workplace support
Maintaining breastfeeding for 6 months can be challenging when women return to work (Gilmour et al, 2013). Currently, UK law does not state that employers must accommodate for breastfeeding mothers; this presents gender inequalities, as women may have to choose between the health of themselves and their child or returning to work (Advisory, Conciliation and Arbitration Service, 2014; Atabay et al, 2015). In comparison, Norway and Sweden have policies allowing unlimited nursing breaks for mothers at work, and have the highest breastfeeding rates in Europe (Save the Children, 2012). There may be economical factors impinging on the uptake of this recommendation in the UK; for example, if a business had a largely female workforce, employees taking extra breaks to breastfeed may lead to reduced productivity, resulting in reduced profits, and consequently, lowering government tax gains (Chow et al, 2011). However, the costs to the employer would be minimal and accommodating breastfeeding practices in the workplace could promote a good relationship with staff, increase job satisfaction and retention rates, having minimal effects on the economy (Chow et al, 2011). Governmental policies based on the WHOs' (2014) and BFIs' recommendations for employers to provide breaks and comfortable areas for women to breastfeed or express milk may encourage breastfeeding practices in the UK (UNICEF UK, 2012). To make this fair and achievable, government incentives could be provided to businesses who implement breastfeeding policies, for example a small tax relief or grant. Not only would this increase health benefits for women and their babies, it may increase the public's knowledge and reduce the stigma of breastfeeding in public, leading to breastfeeding rates increasing in line with leading European countries.
Conclusion
Breastfeeding rates in the UK are much lower than other European countries such as Norway and Sweden, so strategies and innovations to increase breastfeeding rates must be developed (Save the Children, 2012). The International Code of Marketing of Breast-milk Substitutes was one of the pioneering international innovations to increase breastfeeding practices, but the UK does not fully comply with the International Code as it allows the promotion of follow-on formulas (WHO, 1981; Brady, 2012). The Government should close these loopholes and put more financial backing into strategies to increase the rates and maintenance of breastfeeding, such as more postnatal support as recommended by NICE (2013) and the development of incentives for businesses that implement fair breastfeeding policies for their female workforce in-line with WHO (2014) and BFI recommendations (UNICEF UK, 2012). More research must be undertaken on the logistics and practicalities of the financial incentive scheme for breastfeeding mothers including what type of incentive would be best and which health professional would be the lead for this scheme. In addition, research into the effects of the new shared parental leave scheme in the UK on breastfeeding rates and durations should also be undertaken.