
Genital tract sepsis is now the leading cause of direct maternal death in the UK, with the incidence rising since 2006 (Cantwell et al, 2011). Perineal trauma can increase the risk of puerperal infection, potentially leading to sepsis (Cantwell et al, 2011; Kettle, 2011). It is also associated with long- and short-term morbidities such as pain and dyspareunia, stress and urge urinary incontinence, and flatus incontinence (McCandlish et al, 1998; Barrett et al, 2000; Williams et al, 2007). These morbidities can lead to women experiencing complex psychological issues such as social isolation, anxiety, embarrassment and avoidance of intimate contact due to fear of pain (Williams et al, 2005; O'Reilly et al, 2009; Priddis et al, 2013). In addition, women may fear and anticipate pain during the suturing process (Priddis et al, 2013), an intervention which can blight an otherwise satisfying birth experience.
Perineal trauma is classified on the severity of the tear into first, second, 3a, 3b, 3c and fourth degree, depending on the level to which the surrounding tissues are involved. Anterior perineal trauma can also occur to the labia, urethra and clitoris, though this is usually associated with little morbidity (Aasheim et al, 2012). The degree of morbidity is directly related to the degree of perineal injury sustained (Williams et al, 2007; Rådestad et al, 2008; Aasheim et al, 2012). Consequently, it is essential that midwives practise in such a way as to reduce perineal trauma, where possible.
A great deal of research has been conducted into what causes and increases the incidence of perineal trauma (Mayerhofer et al, 2002; Christianson et al, 2003; Albers et al, 2005; da Silva et al, 2012) with many factors being attributed, including primiparity, instrumental birth, ethnicity, heavier babies, maternal age and body mass index. In addition, controllable factors have been found to affect perineal trauma, including birthing techniques and different birth positions (Dahlen et al, 2007; da Silva et al, 2012; Meyvis et al, 2012).
There are published guidelines advising on birth positions (Royal College of Midwives (RCM), 2012a; 2012b; National Institute for Health and Care Excellence (NICE), 2014). However, these identify a lack of robust evidence differentiating between birth positions, including waterbirth when compared with recumbent positions, and the incidence and degree of perineal trauma sustained (RCM, 2012a; 2012b; NICE, 2014). NICE (2014) states that there is no difference in the rate of intact perinea when a supine position is compared with upright positions. However, the guidelines question the methodological quality of the studies used to substantiate their evidence. Consequently, the results should be interpreted with caution. The guidelines also rely on studies that included lateral and semi-recumbent as ‘upright’ positions, which are not recommended by the RCM Better Births Initiative as neither of these positions allow for the assistance of gravity during birth (RCM, 2015).
A Cochrane review (Gupta et al, 2012) examined duration of the second stage of labour, comparing limited birth positions (upright, birth-stool/squatting and birth chair/cushion) with supine/lithotomy positions, excluding waterbirth. However, different upright positions were not compared and perineal trauma was only considered as a secondary outcome. Trauma not requiring suturing was also excluded.
With research demonstrating that birth position affects the rate and degree of perineal trauma (Cluett and Burns, 2009; Gupta et al, 2012; Dahlen et al, 2013), it is important to consider which birth positions midwives are best placed to promote to reduce the degree of trauma women experience. However, no evidence could be found specifically examining data related to this. Consequently, this article will discuss a systematic review that was undertaken to address this, with the following review question:
‘Do different maternal positions at birth affect the incidence and degree of perineal trauma?’
Methods
The review protocol was formulated using the Centre for Reviews and Dissemination's (CRD's) guidance for undertaking systematic reviews (CRD, 2009). An initial literature scoping exercise revealed sufficient literature and no previously conducted reviews with the same review question. A combination of search terms (Table 1) was collated and used in an extensive search of 19 databases and Department of Health publications. Reference lists of relevant articles were hand-searched and known experts in the field contacted. The review was limited to English language and published studies only, due to feasibility constraints, but was not limited by year of publication. Studies that were considered to meet the eligibility criteria (Table 2) based on the title, abstract and subject descriptors were obtained for data synthesis.
| Population | Intervention/Comparator | Outcome |
|---|---|---|
| Labour | Birth/birthing position(s) | Perineal trauma |
| Women | Delivery position(s) | Perineal tear |
| Maternal | Water birth/waterbirth | Perineum |
| Second stage | Pool birth | Perineal injury/ies |
| Birth | Position | Tear |
| Genital tract trauma | ||
| Trauma | ||
| Laceration |
PICOS–patient/problem/population, intervention, comparison/control/comparator, outcomes, study type
| PICOS | Inclusion criteria | Exclusion criteria |
|---|---|---|
| P | Women following a natural vaginal birth | Women following instrumental birth or caesarean section |
| I | Natural/upright birth positions—standing, all fours, on knees, squatting, in water, birth-stool, semi-recumbent position (trunk tilted forwards up to 30° to the horizontal) | Legs in lithotomy, supine/dorsal position, lateral (Sims') position, Trendelenburg position (head lower than pelvis) |
| C | Natural/upright birth positions—standing, all fours, on knees, squatting, in water, on a birth-stool, semi-recumbent position (trunk tilted forwards up to 30° to the horizontal) | Legs in lithotomy, supine/dorsal position, lateral (Sims') position, Trendelenburg position (head lower than pelvis) |
| O | Intact perineum |
Episiotomies |
| S | Quantitative studies | Qualitative studies |
PICOS–patient/problem/population, intervention, comparison/control/comparator, outcomes, study type
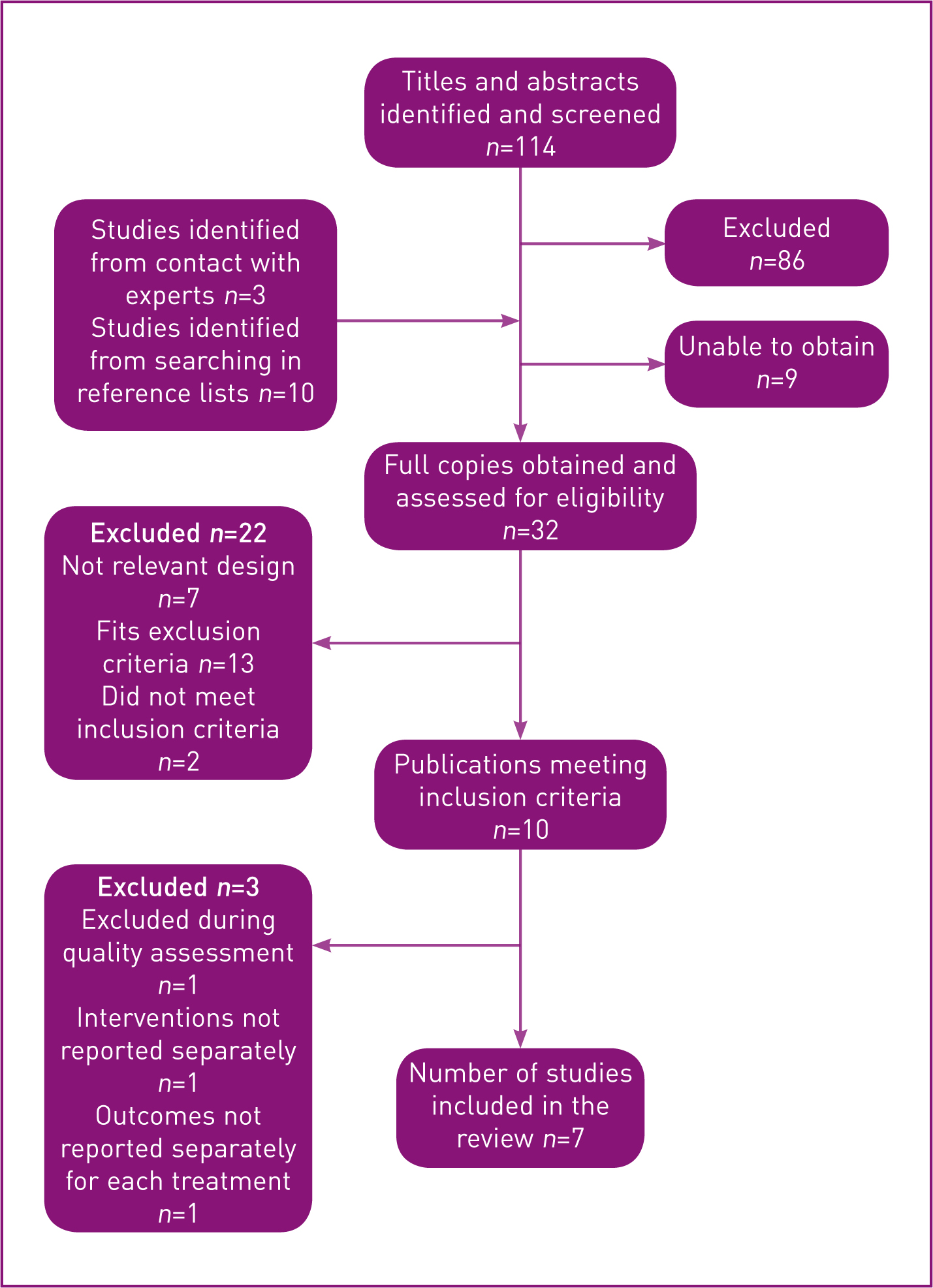
The final search generated 114 citations, and a further 13 studies were discovered through contacting experts and searching reference lists of identified studies. A total of 32 citations were obtained and assessed for eligibility against the inclusion and exclusion criteria, leaving 10 studies suitable to be included in the review (Figure 1). These studies were then subject to quality assessment using the validated checklist from the Critical Appraisal Skills Programme (CASP, 2013). The results from the CASP checklists were presented in a table relating them to the PICOS (problem, intervention, comparison, outcomes, study type) framework, to allow clear comparison of the findings (Table 3). One citation was rejected during this process as the study did not address a clearly focused issue.
| S | P | I | C | |
|---|---|---|---|---|
| Study | Did the trial/study address a clearly focused issue? | Were study participants recruited in an acceptable way/randomised? | Was exposure measured accurately to minimise bias/did blinding occur? | Were the groups similar at the start of the trial/were confounding factors accounted for? |
| Altman et al (2007) Randomised controlled trial (RCT) | Y | Y | N | Y |
| Cortes et al (2011) Cohort study | Y | Y | Y | Y |
| Da Silva et al (2012) * Cohort study | N | Y | ||
| Dahlen et al (2013) Cohort study | Y | Y | Y | Y |
| Gardosi et al (1989) † RCT | Y | Y | N | Y |
| Geissbuehler et al (2004) Cohort study | Y | Y | Y | Y |
| Golay et al (1993) † Cohort study | Y | Y | Y | Y |
| Mollamahmutoğlu et al (2012) Cohort study | Y | Y | Y | Y |
| Shorten et al (2002) Cohort study | Y | Y | Y | Y |
| Soong and Barnes (2005) Cohort study | Y | Y | Y | Y |
CASP–Critical Appraisal Skills Programme; PICOS–patient/problem/population, intervention, comparison/control/comparator, outcomes, study type
Data extraction was undertaken using the Cochrane Collaboration data collection (CCDC) form (Cochrane Collaboration, 2013), a standardised form providing consistency and improving reliability and validity for quantitative studies (Higgins and Deeks, 2011). Risk of bias due to non-randomised studies and poor methodology was considered within the CCDC form using the Cochrane Collaboration's Risk of Bias (CCRB) tool (Higgins et al, 2011). Two studies were excluded due to interventions and outcomes not being reported separately. For transparency of the selection process, excluded studies were recorded in a table, detailing the reason for rejection.
Data synthesis adopted a narrative approach due to the heterogeneity of the included studies (CRD, 2009). Tables were used to assist with the textual narrative, allowing visual exploration of their relationships. As narrative synthesis is inherently a more subjective process than meta-analysis, the author followed the guidance and framework produced by the Economic and Social Research Council (ESRC) methods programme (Popay et al, 2006; Rodgers et al, 2009). The academic supervisor offered ongoing support to reduce the risk of bias.
Findings
Summary of included studies
Table 4 gives an overview of the included studies and Table 5 shows a quality assessment, with the strongest-quality studies to the left and studies with an increased risk of bias to the right of the table. There was vast heterogeneity among the studies, with variability of study design, population, setting, interventions and outcomes. Only one study (Cortes et al, 2011) was undertaken in the UK. The others were conducted in countries across Europe and Australia, all of which have very different maternity systems and practices. Some studies were conducted in hospital labour wards, others in birth centres; the increased risk of intervention in a hospital setting (NICE, 2014) is an important factor for consideration when interpreting results. Some women were attended by midwives, others by obstetricians. These variations—such as episiotomies being standard practice in Turkey, as is being attended by an obstetrician rather than a midwife (Hotun Şahin et al, 2007; Midwifery Today, 2015)—will have influenced results. It is acknowledged that these variations may have influenced the findings of this review.
| Study | Study type | Study characteristics | Participants | Study population | Interventions | Outcomes |
|---|---|---|---|---|---|---|
| Altman et al (2007) | Randomised controlled trial | Swedish hospital delivery ward | 271 | Primiparous | Kneeling and sitting positions | Kneeling and sitting upright during labour were not associated with significant differences in third- and fourth-degree lacerations in normal, healthy women at term |
| Cortes et al (2011) | Retrospective cohort study | UK ‘home from home’ birth unit | 738 | Primiparous | Waterbirth and undefined land birth position | Waterbirth was found to have a greater incidence of third-degree tears (2.5% vs 1.3%) but the overall incidence of intact perineum and perineal trauma following waterbirth and land birth was not statistically significant |
| Dahlen et al (2013) | Retrospective cohort study | Australian alongside birth centre | 6018 | Parity not defined | Waterbirth, all-fours/keeling, semi-recumbent, standing, birth-stool, squatting | Women who gave birth in water compared to positions on land had better perineal outcomes and women who birthed on a birth-stool had a higher rate of perineal trauma |
| Geissbuehler et al (2004) | Cohort study | Swiss hospital | 9518 | Primiparous and multiparous | Waterbirth and land birth positions (bed birth, Maia stool birth, holding onto rope, lying on a mat, supported all-fours and Roma wheel) | Significantly higher rates of ‘no injuries’, first- and second-degree perineal lacerations, vaginal and labial tears were found in the waterbirth group, and significantly more third- and fourth-degree lacerations after spontaneous land births. No difference was found between the two groups for clitoral tears |
| Mollamahmutoğlu et al (2012) | Cohort study | Turkish hospital | 411 | Primiparous and multiparous | Waterbirth and land birth (‘conventional vaginal delivery’) | Perineal laceration rates were higher in the waterbirth group than with conventional vaginal delivery but the authors state ‘however most of these lacerations were minimal’ |
| Shorten et al (2002) | Retrospective cohort study | Australian public hospital | 2891 | Parity not defined | Semi-recumbent, all-fours, kneeling, standing and squatting positions | Alternative birth positions did not perform better than the semi-recumbent position and the squatting position ‘demonstrated least favourable results’ |
| Soong and Barnes (2005) | Prospective cohort study | Australian public hospital | 3756 | Parity not defined | Sitting, semi-recumbent, all-fours, kneeling, standing and squatting positions | Semi-recumbent position was significantly associated with more perineal trauma, while women birthing in the all-fours position were less likely to sustain trauma |
| Types of bias | Studies in order of overall quality assessment including risk of bias Strongest |
||||||
|---|---|---|---|---|---|---|---|
| Altman et al (2007) | Dahlen et al (2013) | Shorten et al (2002) | Mollamahmutoğlu et al (2012) | Geissbuehler et al (2004) | Soong and Barnes (2005) | Cortes et al (2011) | |
| Selection bias— random sequence generation | Low | Low | Unclear | Low | High | Low | Unclear |
| Selection bias— allocation concealment | Low | Low | Unclear | Unclear | Unclear | Low | Low |
| Performance bias | Low | Low | Unclear | Low | Low | Unclear | Low |
| Detection bias | Low | Unclear | Low | Unclear | Unclear | Unclear | Low |
| Attrition bias | Unclear | High* | Low | Low | Low | Low | Low |
| Reporting bias | Low | High* | Low | Low | Low | Low | Unclear |
| Other bias | Low | Low | Low | High | Low | Low | Low |
| Overall risk assessment of bias | Low | High* | Moderate | Moderate | High | Low | Low |
| CASP quality assessment | Good | Good | Good | Good | Good | Adequate | Adequate |
CASP–Critical Appraisal Skills Programme
There was only one randomised controlled trial (RCT) included (Table 4), considered the ‘gold standard’ of research (Altman et al, 2007); the other six were cohort studies, all deemed to be weaker in relation to quality and risk of bias when assessed using the CCRB tool (Higgins et al, 2011; Lodge, unpublished). Authors justified not selecting an RCT from an ethical perspective: that restricting women to certain positions and withholding choices could not be ethically justified. Despite the perceived limitations of cohort designs, the overall assessment of quality was good, so the results can be considered propitiously.
The findings from the systematic review suggest that different maternal positions at birth affect the degree and incidence of perineal trauma.
Waterbirth
This systematic review found more second-degree tears compared to rates of intact perinea and first-degree tears (Cortes et al, 2011; Dahlen et al, 2013), but with more intact perinea in multipara women (Mollamahmutoğlu et al, 2012). Only one study compared waterbirth with different land birth positions (Dahlen et al, 2013), finding it to be protective of perineal trauma in comparison to using a birth-stool and squatting positions but less protective than all-fours/kneeling positions (Dahlen et al, 2013). Compared to land birth in general, an increase in incidence of perineal trauma was found in waterbirth (Geissbuehler et al, 2004; Cortes et al, 2011; Mollamahmutoğlu et al, 2012) contradicting previous research which found no difference in trauma rates between land and waterbirth (Cluett and Burns, 2009).
While Geissbuehler et al (2004) found a reduction in third- and fourth-degree tears with waterbirth in comparison to land birth for primagravid and multigravid women combined, Cortes et al (2011) found an increase. This study, however, only considered nulliparous women and cannot be compared to other included studies considering waterbirth and third- and fourth-degree tears, due to the possible inclusion of episiotomies in their data (Mollamahmutoğlu et al, 2012; Dahlen et al, 2013). Cortes et al's (2011) findings were linked to the length of immersion in water during labour, and the study proposed that water caused an increase in perineal elasticity, shortening the second stage but giving less time for the tissues to stretch. This contradicts Cluett and Burns (2009), who suggested a potential benefit of waterbirth is an increase in elasticity of the birth canal and perineum which may reduce the incidence and severity of tearing.
All-fours and kneeling positions
The greatest incidence of intact perinea was found with all-fours position, with kneeling a close second. Rates above 50% were found in the majority of studies (Shorten et al, 2002; Soong and Barnes, 2005; Altman et al, 2007).
However, Altman et al (2007) and Cortes et al (2011) documented all degrees of perineal trauma as one outcome, and others included anterior trauma in addition (Geissbuehler et al, 2004; Dahlen et al, 2013). Some studies included all tears requiring suturing as one outcome (Shorten et al, 2002; Soong and Barnes, 2005; Mollamahmutoğlu et al, 2012). Consequently, it cannot be examined in any detail whether all-fours and kneeling positions can be protective of different types of perineal trauma.
Sitting, squatting and using a birth-stool
These positions were found to have the highest incidence and degree of perineal trauma, with rates being up to 85.7% for primiparous women (Altman et al, 2007). The rate of second-degree tear (or first and second combined) was around 50% (Shorten et al, 2002; Soong and Barnes, 2005; Altman et al, 2007; Dahlen et al, 2013). Few studies considered anterior trauma but interestingly rates of labial tear were found to be lower with these positions than with waterbirth and other land birth positions (Geissbuehler et al, 2004; Dahlen et al, 2013). This review contradicts previous evidence (Thies-Lagergren et al, 2011) which found no increase in perineal trauma when women used a birth stool. However, this trial restricted its use to 30 minutes. In this context, it was suggested that the high rates of trauma associated with the birth-stool may have been linked to the way it was used in the second stage of labour when progess was slow (Dahlen et al, 2013), assisting in an upright position but possibly causing increased perineal oedema and therefore increased rates of trauma.
Parity
This systematic review aimed to investigate whether perineal trauma and birth position may be influenced by parity. Despite parity being regularly discussed, there were minimal studies included in the review where parity was recorded in relation to birth position, with only one study considering multiparity (Mollamahmutoğlu et al, 2012) and birth positions being limited to kneeling, sitting (Altman et al, 2007), waterbirth (Cortes et al, 2011) and undefined land birth (Mollamahmutoğlu et al, 2012). Without further studies considering parity with birth position, a strong conclusion cannot yet be drawn and practice cannot be influenced.
‘Further research is required into how parity and the length of immersion during waterbirth affects perineal trauma, as well as the safety and practicalities of providing perineal support in active birth positions, including waterbirth’
Implications of findings
The RCM (2015) Better Births Initiative advocates the use of active birth positions to take advantage of gravity. Midwives are advised to encourage women to adopt different positions during labour and birth. Midwives could use the findings from this review when considering which upright position to encourage. Women could be advised that all-fours and kneeling positions may reduce the incidence and degree of perineal trauma. The findings also provide a possible counter-argument to the evidence that waterbirth reduces perineal trauma for nulliparous women (Cluett and Burns, 2009). All-fours and kneeling positions are easily achievable for most women and may particularly benefit women who are reluctant to mobilise away from the bed.
However, it is important to interpret the findings only tentatively due to the other variables that can influence the incidence and degree of perineal trauma and the limitations of this review.
Birth attendants
Some birth attendants are known to have a personal preference for certain birth positions (Shorten et al, 2002; Bodner-Adler et al, 2004) but it is difficult to quantify the influence of this preference on the woman's instinct and choice of position. Although maternal choice was promoted in some studies (Shorten et al, 2002; Geissbuehler et al, 2004; Cortes et al, 2011) it is difficult to say whether the incidence or severity of trauma has been affected as a result of women adopting non-instinctive positions.
Perineal guarding
Perineal guarding is recommended practice by the Royal College of Obstetricians and Gynaecologists (RCOG, 2015) to reduce the incidence of perineal trauma. Only Cortes et al (2011) discussed perineal guarding, suggesting an increase in third- and fourth-degree tears in the waterbirth group may be attributable to a lack of perineal guarding. However, as no other study discussed this practice, it is unclear as to whether not guarding the perineum has affected the rates and degrees of perineal trauma.
Review limitations
Owing to the multiple locations of the trials included, some of the results may not be generalisable to the UK population. One example is the practice of routine episiotomies in the Turkish study (Mollamahmutoğlu et al, 2012). This will reduce the number of documented tears, while the recommendation that episiotomies are not performed in the water will increase the rates of both intact perinea and trauma requiring suturing in waterbirth compared to land birth. Therefore, the findings from this review are tentative and highlight the need for further research to substantiate the implications for practice. Although only one of the included studies was an RCT, this demonstrates the positive ethos of promoting maternal choice of birth position in many countries and birth settings across the world.
A further limitation is the lack of data presented by some of the studies considering parity and the differentiated degrees of perineal trauma. Consequently the reviewer had to make some assumptions about the missing data, though they were not considered significant enough to have affected the overall findings.
Conclusion
This systematic review provides evidence to support midwives advising women antenatally on the benefits of using kneeling and all-fours positions during birth, to increase their chances of an intact perineum while having the gravitational benefits of being upright. These positions would be useful for women who are reluctant to leave the bed and require little physical support from another party. Women should also be alerted to the increased risk of perineal trauma when birthing in a sitting/squatting position or using a birth-stool, and midwives should be mindful of the length of time a woman spends on a birth-stool during the second stage. However, further research is required into how parity and the length of immersion during waterbirth affects perineal trauma, as well as the safety and practicalities of providing perineal support in active birth positions, including waterbirth. In addition, further research is needed into the length of time women spend on birth-stools and/or in the water, and how this affects perineal integrity.
Further research is required in this field, though whether this research should take the form of RCTs or cohort studies is an area for ethical debate. Woodward and Kelly (2004) demonstrated that women are accepting of the idea of participating in RCTs, which may produce the most reliable and unbiased form of research (CRD, 2009). However, encouraging RCTs that restrict women's childbirth choices opposes the Nursing and Midwifery Council (2015)Code, which promotes empowerment and shared decision-making between the midwife and woman. In this context, participating in an RCT would prevent women from adopting instinctive birth positions, a factor that may prove to be protective in itself. To investigate this area fully—including the power of instinct—a majority of good-sized, multi-centred cohort studies, alongside a minority of RCTs, would be required.