
In the course of spontaneous physiological labour, endogenous oxytocin is released from the pituitary gland and initiates uterine contractions. However, when it is deemed medically necessary to induce or augment labour contractions, synthetic oxytocin (Syntocinon) is administered intravenously. Induction or augmentation of labour using Syntocinon is one of the most common interventions for facilitating the progress of labour and birth (Wood et al, 2014). Between 30% and 50% of women receive Syntocinon for augmentation of labour, and 50–70% receive it for induction of labour (Calder et al, 2008). In addition, Syntocinon is often administered intramuscularly after the birth of the baby and during the third stage of labour to prevent post-partum haemorrhage. The administration of Syntocinon depends on a variety of reasons including, but not limited to, maternal medical conditions if they become problematic and necessitate the induction of labour (i.e. hypertension, gestational diabetes, obstetric cholestasis) and fetal indications (i.e. macrosomia, small for gestational age, oligohydramnios, abnormalities) (Declercq et al, 2007).
The use of Syntocinon is regarded as a relatively safe intervention during labour, even for patients who have had a single previous caesarean section in resource-rich developed countries such as France (Sananès et al, 2014), Greece (Rath and Tsikouras, 2015), Australia (Homer et al, 2011) and USA (Landon et al, 2006). Nonetheless, it has been suggested that Syntocinon works differently from endogenous oxytocin, and its effects can be unpredictable (Uvnäs-Moberg, 1998). Animal studies also suggest that the effect of Syntocinon varies depending on the administration site, route, frequency, dose and time (Mota-Rojas et al, 2006). It has been proposed that the unpredictable effects of Syntocinon may interfere with the mother-child attachment, bond and breastfeeding and may affect the child's development (Feldman et al, 2010; Fernández et al, 2012). Here, we review the effect of endogenous oxytocin and Syntocinon on the health and wellbeing of women and their children during labour and after birth, and discuss the benefits of endogenous oxytocin and some adverse effects of Syntocinon.
Endogenous oxytocin and Syntocinon
Endogenous oxytocin and its receptors were first discovered because of their role in inducing labour contractions, the delivery of the baby and stimulating lactation (Fuchs et al, 1984). Endogenous oxytocin is primarily synthesised in the hypothalamus and is then stored in the posterior pituitary gland, where it is released into the bloodstream (Russell et al, 2003; Leng et al, 2008) (Figure 1). The blood–brain barrier prevents the released endogenous oxytocin from re-entering the brain (Mens et al, 1983).
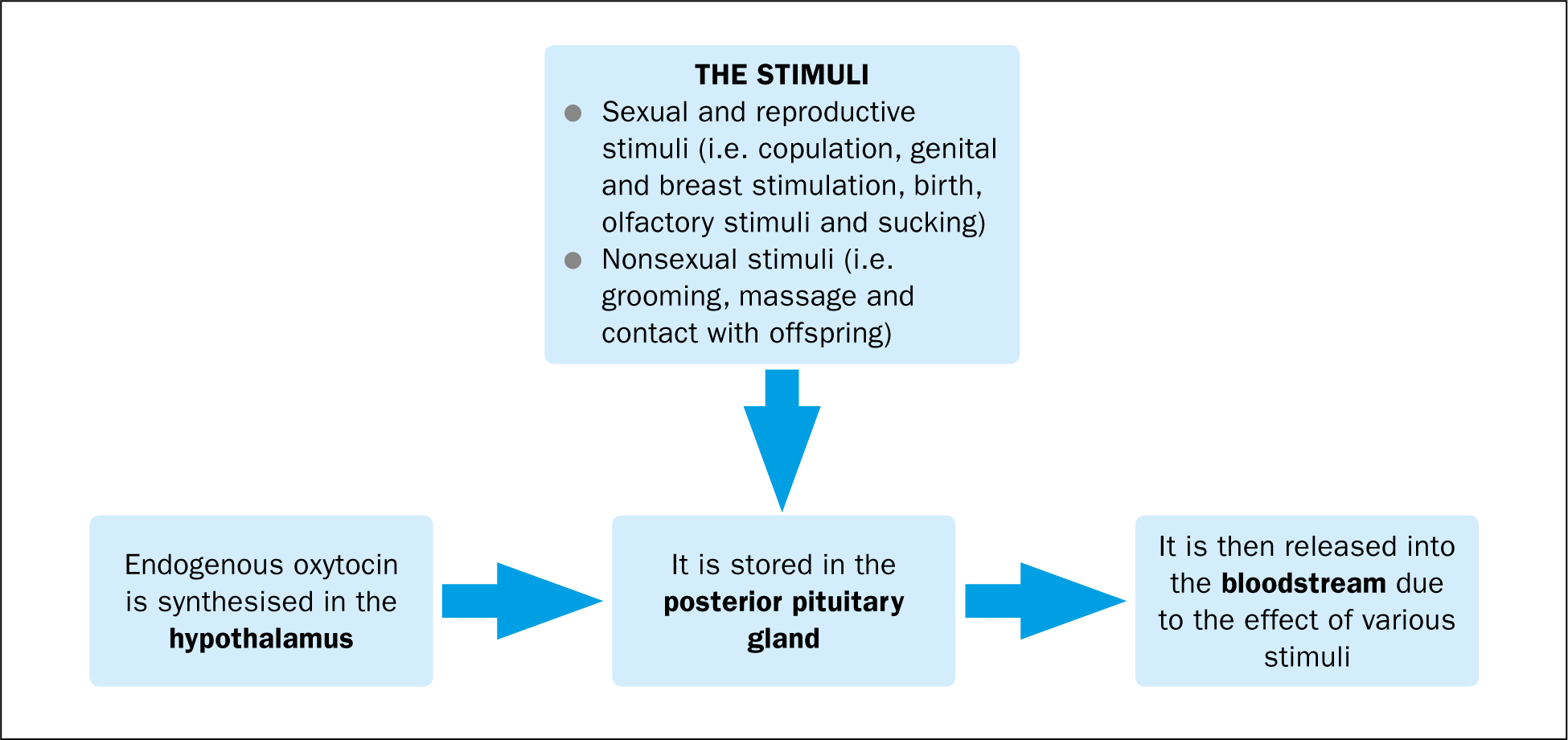
This hormone is also synthesised in the amnion and the chorionic layer of the placenta, and in the decidual layer of the uterus during labour and birth (Cunningham et al, 2010). The release of endogenous oxytocin can be provoked by a variety of stimuli including sexual and reproductive stimuli (i.e. copulation, genital and breast stimulation, birth, olfactory stimuli, and sucking) (Baskerville and Douglas, 2008) and nonsexual stimuli (i.e. grooming, massage and contact with offspring) (Gimpl and Fahrenholz, 2001). The central and peripheral actions of endogenous oxytocin are mediated by its receptors (Russell et al, 2003; Leng et al, 2008).
Endogenous oxytocin has a complex role in the body. It acts as a neurotransmitter in the brain and applies a wide range of central and peripheral physiological effects in women (Cunningham et al, 2010). The spectrum of its effects varies from modulating neuroendocrine reflexes to establishing social and bonding behaviours, such as facilitating milk ejection, uterine contractions, birth, copulation, maternal behaviours, partner and offspring preference and social contacts (Feldman et al, 2010).
Endogenous oxytocin has unique interactions with the body and does not act in the same way as Syntocinon. Although Syntocinon has a well documented role during labour and can be a life-saving intervention for many women (Cunningham et al, 2010), it can impede the delicate orchestration of natural hormones of the mother and baby during and after birth, which is not free of risks (Fernández et al, 2012; Weisman et al, 2015). We discuss details of these changes in the following sections.
Preparation of fetal neurons for birth
Maternal endogenous oxytocin may help prepare the fetus for birth and may have a role in protecting the fetal brain during labour and birth. According to animal studies (Tyzio et al, 2006; Khazipov et al, 2008), maternal oxytocin crosses both the placental barrier and fetal blood–brain barrier during labour. It enters the fetal brain and prompts a transient switch in the action of the neurotransmitter gamma-aminobutyric acid (GABA) (Khazipov et al, 2008), changing GABA from having an excitatory to an inhibitory effect. GABA then inhibits fetal cortical neurons, reduces fetal brain activity for the duration of labour and delivery, and helps decrease the vulnerability of the fetal brain to hypoxic damage during birth. These changes start the day before the onset of physiological labour and have maximal effect during the second stage of labour. The effects of these GABA-induced changes include decreased central blood flow, decreased oxygen requirement and reduced vulnerability to hypoxic brain damage (Tyzio et al, 2006; Khazipov et al, 2008).
There is, however, disagreement about whether peripherally administered Syntocinon has the same effects, crosses the fetal blood–brain barrier and alters the neuronal actions of the fetal nervous system (Churchland and Winkielman, 2012). In theory, based on the pharmacological properties of Syntocinon, this drug is not able to cross the blood–brain barrier because of its large molecular size and hydrophilic nature. However, some animal studies have found low levels of Syntocinon in the fetal brain after parenteral administration, and that administration of high-dose synthetic oxytocin (Ceanga et al, 2010) or the oxytocin antagonist atosiban (Tyzio et al, 2006) block the oxytocin receptors, reducing the neuroprotective effects of endogenous oxytocin and increasing the fetus' vulnerability to hypoxic brain damage.
Uterine contractions and pain management
The role of endogenous oxytocin in stimulating uterine contractions during the expulsive phase of labour and delivery is very well known (Russell et al, 2003; Leng et al, 2008). According to animal studies (Young et al, 1997), during the body's preparation for the physiological onset of labour, the rising oestrogen level during the last weeks of pregnancy increases the number and sensitivity of oxytocin receptors in the uterus leading up to birth. These changes are accompanied by an increase in the oxytocin receptors in the hypothalamus and olfactory bulbs. This increase, in turn, raises the sensitivity of the hypothalamic and olfactory neurons to endogenous oxytocin and prepares the body for birth. It has been shown that the descent of the baby during labour stimulates stretch receptors in the lower vagina and cervix. This triggers a pulsatile release of endogenous oxytocin from the posterior pituitary gland into the bloodstream and stimulates uterine contractions (also known as the Ferguson reflex) (Russell et al, 2003; Leng et al, 2008).
Endogenous oxytocin blocks the β-adrenergic receptors and decreases clearance of endorphins, especially the β-endorphin. This process raises the level of plasma endorphins, increases their binding to opioid receptors on the uterus and results in pain reduction. This can relieve some of the pain associated with uterine contractions and labour (Saisto et al, 2004).
During natural labour, endogenous oxytocin reaches a peak at birth, when it stimulates the fetal ejection reflex and allows for an easier delivery, as shown in animal studies (Gilbert et al, 1994). In addition, an increase in the number of oxytocin receptors and in uterine contractility helps the uterus to contract after delivery, resulting in placental separation and expulsion (Blanks and Thornton, 2003).
Endogenous oxytocin and Syntocinon are similar in terms of binding to oxytocin receptors on the uterine muscles, but Syntocinon can have unpredictable effects on the body. This could be partly due to the physiological differences in oxytocin receptors during induction of labour with Syntocinon. Unlike endogenous oxytocin, Syntocinon is administered continuously at various doses via an intravenous cannula (Cunningham et al, 2010). If labour has not started physiologically, fewer oxytocin receptors exist in the uterine muscles and, therefore, higher doses of Syntocinon (10–16 mU/minute) are administered to induce labour (Fuchs et al, 1983). This is markedly higher than the dose required for augmentation of labour (4–6 mU/minute) when physiological labour has already started and enough oxytocin receptors exist (Fuchs et al, 1983).
Large doses of Syntocinon can increase the resting tone of the uterine muscle by creating more frequent, longer and stronger contractions. An increased resting tone of the uterine muscle can reduce blood flow to the uterus and placenta, as shown in preliminary animal studies (Brotanek et al, 1969) and result in myometrial ischemia and increased pain sensation (Lowe, 1996). The ischemia may in turn compromise fetal replenishment of blood and oxygen between contractions and result in abnormal fetal heart rate patterns, fetal distress and even uterine rupture (Bell et al, 2014). These events may occur because the constant administration of Syntocinon does not allow its levels to decrease between contractions as much as would occur for endogenous oxytocin in physiological labour. The physiological pulsatile secretion of endogenous oxytocin, along with increased oxytocinase production, helps the uterine muscles rest between contractions and improves fetal blood supply (Nomura et al, 2005).
The increased pain sensation that occurs with Syntocinon use is not only because of vigorous myometrial ischemia but may also be due to the inhibitory effects of Syntocinon on the release of endorphins in the brain. Genazzani et al (1985) compared β-endorphin levels in women in spontaneous labour with women who received Syntocinon to stimulate uterine contractions. They found that in women in spontaneous labour, the plasma levels of β-endorphin increased significantly throughout labour until delivery. However, the β-endorphin levels remained constant or lower in women who received Syntocinon. Genazzani et al reported that the lower levels of β-endorphin in women who received Syntocinon to stimulate uterine contractions could have been related mostly to the primary uterine hypocontractility rather than to intravenous Syntocinon administration. However, they pointed out that using Syntocinon to augment or induce labour can result in tocophobia (anxiety and fear of childbirth) which might be associated with lower β-endorphin levels in those women. Results of the study by Genazzani et al were supported by a later study (Petraglia et al, 1986) suggesting that administration of Syntocinon (0.4 μg/min for 120 min) could inhibit the rise of β-endorphin in stressful situations in healthy humans.
Lactation and breastfeeding
Endogenous oxytocin continues to play an important role in lactation and breastfeeding after stimulating uterine contractions during labour and delivery. Pulsatile secretion of endogenous oxytocin stimulates the release of prolactin, a hormone produced by the lactotroph cells in the pituitary gland. Prolactin is responsible for milk production (Nissen et al, 1996). Nipple stimulation during breastfeeding sends a signal via the spinal cord to the hypothalamus. This results in the release of oxytocin from the pituitary gland into the bloodstream. Endogenous oxytocin then binds with its receptors on the smooth muscle cells of alveoli in the mammary glands, resulting in the milk-ejection reflex, also known as the forceful let-down reflex, with milk ejected from the mammary glands into the ducts and cisterns (Leng et al, 2008).
Endogenous oxytocin facilitates breastfeeding by making the mother more relaxed and more confident about successfully breastfeeding her baby. Research has shown that women who breastfeed their babies are calmer and report lower stress levels than women who formula-feed their babies, which has been attributed to higher levels of plasma oxytocin in breastfeeding women (Schwarze et al, 2014). In addition to the psychological benefits of breastfeeding, the release of endogenous oxytocin during breastfeeding induces mild but often painful uterine contractions that help decrease the size of the uterus and postpartum lochia (Cunningham et al, 2010).
Syntocinon can affect the mother and alter initiation of breastfeeding. Administration of high doses of Syntocinon during labour impairs the pulsatile secretion of endogenous oxytocin, desensitises or downregulates oxytocin receptors, decreases their responsiveness, and finally alters the maternal neural architecture. In the study by Phaneuf et al (2000), myometrial samples were taken from women before the onset of labour, after the onset of spontaneous labour and after induced or augmented labour, and were tested for the quantity and sensitivity of oxytocin receptors. Results showed that although receptor desensitisation occurred in both spontaneous and induced or augmented labour, in women who had undergone induced or augmented labour there was a significant reduction in oxytocin binding that was associated with a longer duration of Syntocinon infusion. In addition, the concentration of oxytocin mRNA was much lower in induced or augmented labour than in spontaneous labour.
Syntocinon molecules resemble vasopressin (an antidiuretic hormone). Since Syntocinon is often administered in relatively high doses during labour and after birth, it can have antidiuretic effects and can lead to breast engorgement and complicated breastfeeding. Another way that Syntocinon can affect breastfeeding success is that the strong, painful contractions it initiates during labour can raise the level of stress and anxiety in the mother (Jonas et al, 2009). The study by Jonas showed that oxytocin infusion uplifts the reactivity of the hypothalamic–pituitary–adrenal (HPA) axis, which controls the body's stress response (Jonas et al, 2009) and results in delayed onset of lactogenesis and unsuccessful breastfeeding (Matias et al, 2010).
The association between Syntocinon and impaired breastfeeding is believed to be dose-dependent (Olza Fernández et al, 2012). Fernandez et al. reported an association between higher Syntocinon doses during labour and impaired infant sucking after birth. In addition, the rate of exclusive breastfeeding for babies at 3 months of age was higher in women who had received a markedly lower average dose of Syntocinon during labour (Fernández et al, 2012). The study by Beebe et al (2007) revealed that compared with spontaneous labour and birth, the Apgar score at one minute was more likely to be less than three in induced labour. Matias et al (2010) reported that a low Apgar score can delay the onset of lactogenesis and interfere with successful breastfeeding. Similarly, a multinational study (Guerra et al, 2009) found that children born during induced labour are at greater risk of a low Apgar score at five minutes than children born during spontaneous labour. This study suggested that inducing labour when labour is not indicated may be the likely cause of adverse fetal outcomes. Nevertheless, these findings are not supported by reports of other research indicating no significant association between the use of Syntocinon for induction of labour and low Apgar scores at 5 minutes after birth (Gülmezoglu et al, 2006).
The negative impacts of Syntocinon on breastfeeding may be due to a low Apgar score and also a result of other adverse neonatal outcomes associated with induction or augmentation of labour, such as hyperbilirubinaemia (Trotman and Henny-Harry, 2012), admission to the neonatal intensive care unit (NICU) (Clark et al, 2009). These impacts may be because successful breastfeeding requires the child to be alert with coordinated sucking, swallowing and breathing and not being separated from the mother (Romano and Lothian, 2008).
Maternal behaviours and child development
Human studies suggest that central oxytocin may be involved in behavioural adaptations to the maternal role, parenting behaviour, social development and affectionate touch (Feldman et al, 2010). It enhances positive feelings and memory for facial identity that will help mother to recognise her newborn. This system, which depends not only on the release of oxytocin but also on oxytocin receptor distribution, becomes particularly important at birth, when the primary bond is formed between mother and baby (Savaskan et al, 2008).
Administration of Syntocinon during labour hinders the pulsatile secretion of endogenous oxytocin, which may have a lasting effect. Animal studies have shown that the brain is sensitive to hormonal imprinting effects. Therefore, the manipulation of the hormone system at birth may predict lifelong changes in social behaviours and their associated repertoire (Bales et al, 2013). This theory is supported by other animal studies indicating that hormonal imprinting takes place in neonates when the developing receptors and their target hormones meet for the first time (Csaba, 2000). Evidence suggests that exposure to Syntocinon during birth may change the infant's DNA methylation, and these changes may affect the neuropeptide systems of the child's brain (Emberti Gialloreti et al, 2014). Animal studies have also shown that patterns of maternal behaviour, such as licking and grooming, shape the neurochemical organisation of oxytocin in the infant's brain during the early stages of life (Kappeler and Meaney, 2010).
Low levels of plasma endogenous oxytocin during the first and third trimester of pregnancy, as well as inhibited endogenous oxytocin during labour, have been shown to correlate with maternal postpartum anxiety and depression symptoms (Kroll-Desrosiers et al, 2017), minimal affectionate touch and low levels of attachment behaviour and social synchrony (Feldman, 2012). This extragenomic dissemination explains a bio-behavioural feedback circle: maternal oxytocin regulates the mother's care-giving behaviours, which in turn outlines the infant's oxytocin through distinctive parenting behaviour (Champagne, 2008).
Statistical analysis of more than half a million births in the USA revealed a link between induction or augmentation of labour and increased odds of the child attending an educational programme for children with special needs, particularly autism spectrum disorders (Gregory et al, 2013). The researchers, however, suggested further research on the association of induction and/or augmentation of labour with autism, as it was unclear whether this association was because of induction or augmentation of labour, the medications used during labour, the underlying medical and obstetric conditions, or acute intrapartum events (Gregory et al, 2013). In contrast to these findings, two earlier studies showed no association between antepartum use of Syntocinon and a subsequent diagnosis of autism in the child (Fein et al, 1997; Gale et al, 2003). It is difficult to interpret the validity and generalisability of the results of the two latter studies because of the small sample size in one study (Gale et al, 2003), and missing data on gender as a variable in data analysis of the other study (Fein et al, 1997), as risk has been reported to be higher in male children (Weisman et al, 2015).
As mentioned earlier, the risk of a low Apgar score is higher in newborns whose mothers have received Syntocinon during labour. A low Apgar score is associated with a higher chance of admission to the NICU and postpartum separation of mothers and infants. This early separation can have negative short- and longer-term effects, such as disruption of successful initiation of breastfeeding, lack of skin-to-skin contact, increased levels of stress hormones, hypoglycaemia and hypothermia in the infants, and shortfalls in maternal hormones and role adaptations affecting the mother–infant attachment (Moore et al, 2012).
Conclusion
Endogenous oxytocin has extensive effects on the brain and body during reproduction. In labour and birth, it optimises the transition to the postpartum period in the mother and infant. Endogenous oxytocin is released into the maternal bloodstream and causes rhythmic uterine contractions, imposes soothing and analgesic effects in mothers and infants throughout labour and the postpartum period, has positive feedback on its release, accelerates the progress of labour, increases postpartum maternal adaptations, and enhances satisfaction with infant care and contact. The pre-labour rise in oxytocin receptors in the brain and the uterine muscles maximises these effects.
Intravenous Syntocinon administered during labour can facilitate the birth of the baby, but it has some adverse effects on mothers and their infants (Table 1). Although there is a lack of high-quality up-to-date human research, it has been suggested that Syntocinon hinders the pulsatile secretion of endogenous oxytocin and may disrupt the beneficial effects of endogenous oxytocin. Syntocinon use may have short- and longer-term effects in mothers and babies, such as increased perception of pain during labour, impaired breastfeeding, disturbed maternal behaviours and changes in the child development. Considering these potentially life-changing effects on women, further human studies are required.
| Endogenous oxytocin | Syntocinon |
|---|---|
| Modulating neuroendocrine reflexes | Uterine contractions |
| Preparation of fetal neurons for birth | Birth of the baby |
| Uterine contractions | Potentially increasing the fetus's vulnerability to hypoxic brain damage |
| Birth of the baby | Myometrial ischemia |
| Facilitating milk ejection and breast-feeding | Increased sensation of pain |
| Maternal behaviours (behavioural adaptations to the maternal role; positive feelings and memory for facial identity) | Likelihood of abnormal fetal heart rate patterns, fetal distress and uterine rupture |
| Bonding and attachment | Impaired lactation and breast-feeding |
| Establishing social behaviours | Maternal postpartum anxiety and depression symptoms |
| Partner and offspring preference | Minimal affectionate touch and low levels of attachment behaviour and social synchrony |
Further to this, midwives and other childbirth professionals need to exercise caution in using this drug. They should keep their knowledge about Syntocinon up to date, and inform pregnant women about the similarities and differences between endogenous oxytocin and Syntocinon and their powerful role through labour, birth and beyond. In order to minimise the consequences of Syntocinon use, pregnant women should be told about the potential effects of Syntocinon. This will allow women to make informed choices about induction of labour and to seek support when required. Pregnant women should, however, know that some women need induction or augmentation of labour due to fetal, maternal or obstetric indications and there may be few alternatives to Syntocinon (Mishanina et al, 2014).
Childbirth should be a positive experience for women and their families. It is the responsibility of healthcare providers to equip themselves and women with appropriate knowledge to minimise negative outcomes and promote quality of life for women and their families. To this end, healthcare professionals should promote normality and help labouring women boost their endogenous oxytocin levels to facilitate the birth. Breast/nipple stimulation and sexual activity have been suggested to help promote natural physiological labour and birth. Oxytocin is known as the hormone of love and is secreted during sexual activity. Although research into the role of sexual intercourse as a method of induction of labour is tentative (Kavanagh et al, 2001), it has been shown that breast/nipple stimulation and having sex or an orgasm are positively correlated with higher plasma levels of oxytocin (Salonia et al, 2005). The level of vaginal lubrication and sexual arousal in women, which is correlated with higher levels of oxytocin, is enhanced by stimulating the nipples and breasts (Levin and Meston, 2006). Furthermore, the release of oxytocin into the bloodstream reaches a peak during orgasm resulting in involuntary rhythmic uterine contractions (Komisaruk et al, 2006). In addition to the release of oxytocin during sexual activity and orgasm, semen contains prostaglandins (PGs) that act as modulators, fine-tuning the system (Hertelendy and Zakár, 2004). Research has shown that the concentration of PGs in cervical mucus samples taken within several hours of sexual intercourse is 10–50 times greater than normal (Huleihel et al, 1999). In addition, the amount of PGE delivered into the vagina during sexual intercourse is similar to the amount of the PGs that stimulate cervical ripening and onset of labour (Nuutila and Kajanoja, 1996). These findings, on the other hand, are interesting because a Cochrane review has reported that sexual intercourse does not promote cervical ripening (Kavanagh et al, 2001). It seems logical to conclude that any recommendations given to pregnant women should be on a case by case basis and according to individual circumstances.
Other activity that may assist with natural physiological labour and birth is walking or ambulating during labour. Systematic review of the literature has shown that the duration of first stage of labour is almost 1 hour and 20 minutes shorter for women who are in upright position or walk around during labour (Lawrence et al, 2013). Although there is a need for further research to validate these results for all women in labour, it seems acceptable to advise women to ambulate during labour if they feel comfortable doing so and there are no maternal or fetal concerns requiring the women to stay in bed.
Complementary therapies have attracted the attention of health professionals during recent decades. Despite their popularity, there are controversial reports in the literature regarding their efficacy in inducing labour contraction and decreasing the duration of labour. Acupressure has been reported in clinical trials to reduce the length of the first stage of labour (Mollart et al, 2015). Nevertheless, further research is required to explore its efficacy in the onset of labour, duration of labour and uterine contractions. Similarly, results of systematic reviews have shown very limited benefit from acupuncture (Smith et al, 2013) and no benefit from homeopathy (Smith, 2003) to induce labour. Their effectiveness has not been shown and there is insufficient evidence to support their use as methods of induction of labour. Before suggesting implications for clinical practice, well-designed trials are required to investigate the role of complementary therapies in labour induction.
In conclusion, providing pregnant women with enough appropriate information will help them make informed decisions about how to manage their labour. In consultation with their midwives or doctors, it can help them choose practical ways of working with their body and hormones, in particular endogenous oxytocin, to maximise their chance of having a physiological birth, free of interventions and side effects.